Dosing schedule modification is a key strategy for neutropenia management during venetoclax therapy. In the VIALE-A study, 76% of long-term responders receiving VEN/AZA had a modified 21 day/cycle venetoclax schedule for grade 4 cytopenia following blast clearance [5]. In a post hoc analysis of VIALE-A, among 185 responders, 74% required a delay (median 10 days) before the next cycle after blast clearance [6]. Similar real-world observations have been reported, with earlier bone marrow assessment recommended to inform venetoclax dosing modifications [7]. In our interim analysis, the median duration of venetoclax treatment was 21.0 days/cycle, and venetoclax dose holds were 8.5–15.0 days during Cycles 2–8, consistent with previous reports [6, 7].
According to clinical practice guidelines, use of anti-infective prophylaxis is recommended based on the patient’s history and individual scenario such as severe neutropenia [8, 9]. In this study, 73.3% of patients received antifungal prophylaxis, with use highest (65.8%) in Cycle 1 and then gradually decreasing with subsequent cycles but remaining high (Cycle 10: 57.1%). Antifungal use to treat infection was limited. Venetoclax dose reductions are required in the presence of cytochrome P450 3A (CYP3A) inhibitors including azole antifungals. A post hoc analysis of VIALE-A showed that use of CYP3A inhibitors does not impact outcomes [10]; however, toxicity of antifungals may be a concern when used broadly [11].
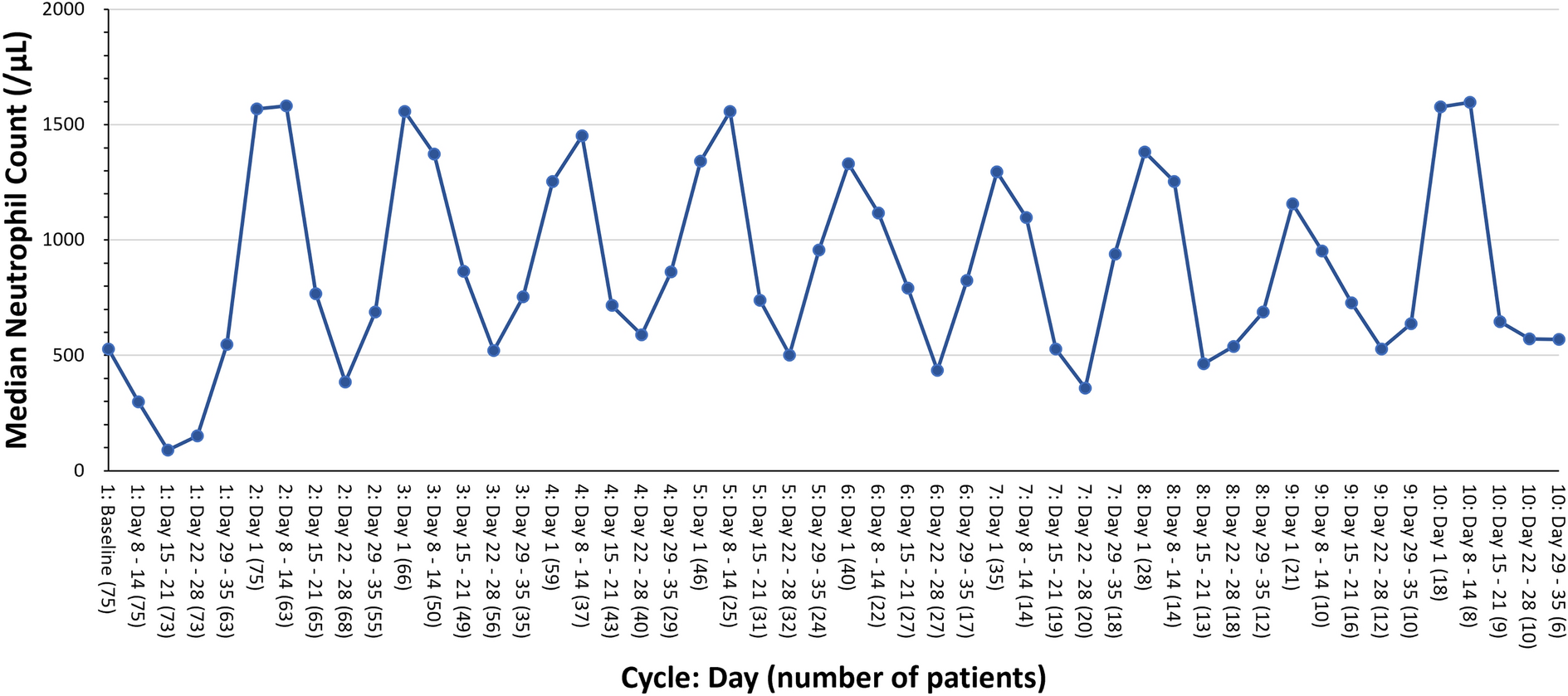
In Cycle 1, nadir neutrophil count decreased to < 500/µl during Days 8–28 but recovered to > 500/µl by Days 29–35. From Cycle 2 onward, although nadir neutrophil count was < 500/µl in some cycles, neutrophil count improved to > 500/µl by the next week. Japanese guidelines for deep-seated mycosis do not recommend antifungal prophylaxis when neutrophil count is anticipated to be < 500/µl for under 7 days [12]. Some recent studies of venetoclax plus HMA [13] and VEN/AZA [14] for newly-diagnosed AML reported relatively lower rates of antifungal prophylaxis use of 17% and 6.9%, respectively, and a low frequency of probable/proven invasive fungal infections (3.1% and 5.6%, respectively). Other studies reported relatively higher rates of antifungal prophylaxis use in newly-diagnosed AML (67.2% with venetoclax plus HMA [15] and 46% with VEN/AZA [16]) and a low frequency of invasive fungal infections (5.1% and 3.2%, respectively), with no significant differences in the incidence of invasive fungal infections based on antifungal prophylaxis use. Considering reports on the heterogenous incidence of invasive fungal infections and antifungal prophylaxis use in clinical practice, as well as the neutrophil recovery observed in this study, broader use of antifungal prophylaxis may not be required for patients treated with VEN/AZA but reserved for patients at higher risk [11].
Our analysis showed that concomitant G-CSF may be related to more venetoclax treatment cycles. In the VIALE-A study, G-CSF was used in 50% of VEN/AZA-treated patients who achieved remission, with or without incomplete hematologic recovery [17]. G-CSF use was not associated with new safety signals and had no negative impact on DOR or OS among venetoclax-treated patients. Delays between treatment cycles were shorter in patients who received post-remission G-CSF [17]. Accelerated neutrophil recovery could allow for earlier initiation of the next cycle of treatment, which could result in maintaining efficacy of venetoclax.
This study has potential limitations. Due to the retrospective nature of the real-world evidence, treatment (dosing patterns of VEN/AZA), supportive care including G-CSF and antifungal prophylaxis and timing of bone marrow evaluations varied among patients and sites. In addition, since this was an interim analysis, results may change with subsequent analyses. The effects of sex on venetoclax treatment outcomes were not assessed in this interim analysis; however, given that there are important sex-based differences in the incidence, molecular profile, and prognosis of AML [18, 19], sex-disaggregated analyses will be considered in the final analysis publication.
Finally, the quality of real-world data can be inconsistent, with potential issues in data collection, completeness, and accuracy, which in turn may affect the reliability of real-world findings. On the other hand, real-world evidence reflects the effectiveness of treatments in a broader range of patients and clinical settings than those captured in randomized clinical trials. It provides insights into how drugs perform in everyday clinical practice, beyond the controlled environments of randomized clinical trials. Real-world evidence informs real-world treatment patterns, sequencing, and adherence; offers practical insights into the management of diseases in day-to-day practice; and can reveal variations in treatment approaches and outcomes across different regions and healthcare settings [20].

Comments (0)