
Remember me
In total, 2260 patients and 437 caregivers accessed the appropriate survey. The patient survey was completed by 202 patients (bladder cancer, N = 29 [14.4%]; gastric cancer, N = 19 [9.4%]; HN cancer, N = 21 [10.4%]; melanoma, N = 45 [22.3%]; NSCLC, N = 25 [12.4%]; RCC, N = 21 [10.4%]; TNBC, N = 42 [20.8%]; Table 1). Mean age of participating patients was 57.1 years; 70.8% reported being female and 71.8% reported being white. Among patients who were excluded from the survey (N = 2049), most (N = 1502 [73.3%]) were excluded from participation as a result of not having a cancer of interest.
Table 1 Patient demographics and clinical characteristicsThe caregiver survey was completed by 100 caregivers (bladder cancer, N = 15 [15.0%]; gastric cancer, N = 13 [13.0%]; HN cancer, N = 10 [10.0%]; melanoma, N = 17 [17.0%]; NSCLC, N = 15 [15.0%]; RCC, N = 11 [11.0%]; TNBC, N = 19 [19.0%]; Table 2). Mean age of participating caregivers was 51.7 years, and 71.0% were female and 59.0% were white. Among caregivers who were excluded from the survey (N = 337), the most common reason for exclusion (N = 154 [45.7%]) was the cared-for person’s not having a cancer of interest.
Table 2 Caregiver demographics and clinical characteristics of cared-for personsAcross cancer types evaluated, the mean (SD) time from initial early-stage diagnosis to survey participation was 7.4 (5.7) years and from first recurrence to survey participation 3.5 (3.3) years. The longest mean (SD) times from initial early-stage cancer diagnosis to survey participation were for patients with melanoma (9.2 [7.8] years), TNBC (8.6 [5.9] years), NSCLC (7.4 [5.2] years), and HN cancer (7.4 [5.5] years), and the shortest times for those with RCC (5.2 [2.3] years), bladder cancer (5.5 [2.6] years), and gastric cancer (5.7 [4.2] years). The longest mean (SD) times from first recurrence to survey participation were for patients with melanoma (4.4 [4.5] years), TNBC (4.1 [3.8] years), NSCLC (3.8 [2.7] years), and HN cancer (3.6 [3.7] years), and the shortest times for those with gastric cancer (2.2 [1.2] years), RCC (2.3 [1.7] years), and bladder cancer (2.4 [1.7] years). Additional information on patient and caregiver demographics and clinical characteristics has been published separately [26].
Patient SurveyEQ-5D-5LAt the time of the survey (i.e., post-recurrence), the mean (SD) patient EQ-5D-5L index score was 0.50 (0.44) and VAS score was 57.8 (22.9) (Fig. 1). Mean index scores were found to differ significantly (P = 0.013) across tumor types, with patients diagnosed with RCC (0.40 [0.44]), NSCLC (0.36 [0.58]), gastric tumors (0.35 [0.53]), and HN tumors (0.35 [0.49]) having the lowest QoL scores and those diagnosed with melanoma (0.69 [0.31]) and TNBC (0.58 [0.31]) having the highest. Significant differences in mean (SD) VAS scores were also seen across tumor types, with the lowest QoL scores reported for patients with RCC (53.5 [21.6]), gastric cancer (52.8 [28.6]), and HN cancer (50.9 [22.0]), and the highest QoL scores reported for patients with melanoma (68.3 [18.4]) and TNBC (60.8 [16.9]).
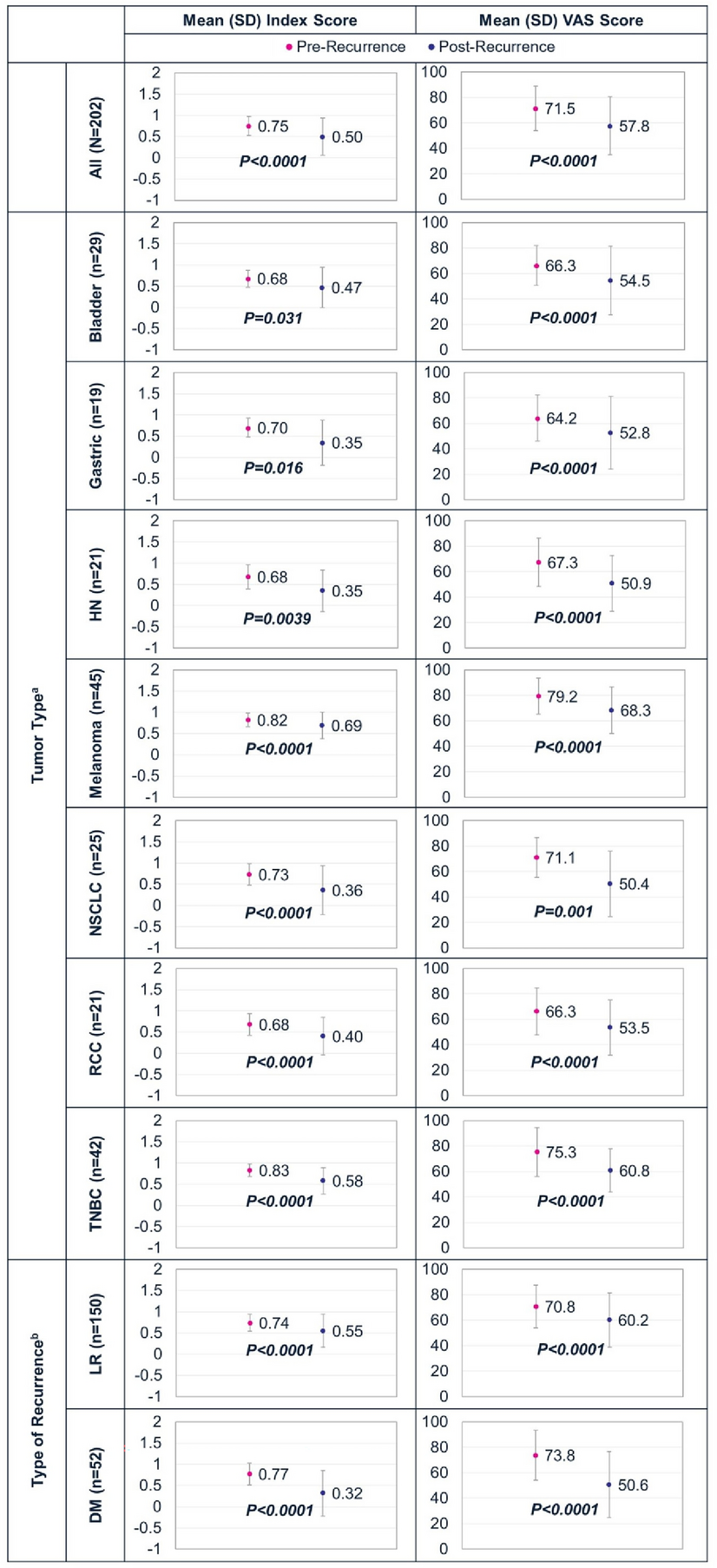
Fig. 1
Change in mean (SD) EQ-5D index and VAS scores from pre-recurrence to post-recurrence for all patients, by tumor type, and by type of recurrence. aStatistically significant differences were seen in post-recurrence EQ-5D-5L index scores across all tumor types (P = 0.013). bStatistically significant differences were seen in post-recurrence EQ-5D-5L index (P = 0.017) and VAS (P = 0.030) scores between patients with locoregional and distant/metastatic recurrences. DM distant/metastatic, HN head and neck, LR locoregional recurrence, NSCLC non-small cell lung cancer, RCC renal cell carcinoma, SD standard deviation, TNBC triple-negative breast cancer, VAS visual analog scale
Compared with patients with a locoregional recurrence, patients with a distant/metastatic recurrence had significantly worse mean (SD) index (0.32 [0.54] vs 0.55 [0.39], P = 0.017) and VAS scores (50.6 [25.9] vs 60.2 [21.4], P = 0.030) (Fig. 1).
From pre-recurrence to post-recurrence, significant decreases were seen in the mean (SD) EQ-5D-5L index (0.75 [0.22] vs 0.50 [0.44], P < 0.0001) and VAS (71.5 [17.6] vs 57.8 [22.9], P < 0.0001) scores for patients when all tumor types were evaluated together and when each tumor type was evaluated separately (Fig. 1). Decreases in QoL were also evident from pre-recurrence to post-recurrence in EQ-5D-5L index and VAS scores irrespective of whether the patient had a locoregional (index: 0.74 [0.20] vs 0.55 [0.39], P < 0.0001; VAS: 70.8 [16.9] vs 60.2 [21.4], P < 0.0001) or distant/metastatic recurrence (index: 0.77 [0.26] vs 0.32 [0.54], P < 0.0001; VAS: 73.8 [19.6] vs 50.6 [25.9], P < 0.0001). However, a greater absolute difference from pre-recurrence to post-recurrence was seen in patients with a distant/metastatic compared with locoregional recurrence (mean index score absolute difference 0.45 vs 0.19; mean VAS score absolute difference 23.2 vs 10.6).
The pre-recurrence to post-recurrence analyses by type of recurrence and by tumor type generally showed decreases in EQ-5D-5L index and VAS scores for all tumor types regardless of type of recurrence. However, greater decreases in QoL scores were seen from pre-recurrence to post-recurrence across all tumor types for patients with a distant/metastatic compared with a locoregional recurrence (Fig. 2).
Fig. 2
Change in mean (SD) EQ-5D-5L index and VAS scores from pre-recurrence to post-recurrence for patients with locoregional and distant/metastatic recurrences by tumor type. HN head and neck, NSCLC non-small cell lung cancer, RCC renal cell carcinoma, SD standard deviation, TNBC triple-negative breast cancer, VAS visual analog scale
Information on the EQ-5D-5L individual domain health states for patients can be found in Sect. 2.1.1 of the electronic supplementary results and Fig. S1.
EORTC QLQ-C30Across all patients, the post-recurrence mean (SD) global health status/QoL score for the past week was 52.2 (25.8) (Fig. 3). Global health status/QoL scores varied significantly (P = 0.042) across tumor types, with the lowest scores for patients with HN tumors (42.9 [26.0]), NSCLC (43.7 [30.2]), and gastric tumors (44.7 [32.4]) and the highest scores for patients with melanoma (62.6 [22.2]).
Fig. 3
Mean (SD) post-recurrence EORTC QLQ-C30 functioning domain scores for all patients, by tumor type, and by type of recurrence. a Wilcoxon rank sum test. DM distant/metastatic, EORTC QLQ-C30 European Organisation for Research and Treatment of Cancer Core Quality of Life questionnaire, HN head and neck, LR locoregional recurrence, NSCLC non-small cell lung cancer, RCC renal cell carcinoma, SD standard deviation, TNBC triple-negative breast cancer
Significant differences in financial difficulties (P = 0.010) as well as in all domain scores (Fig. 3) were seen across all tumor types, including the following symptom scores: fatigue (P < 0.001), nausea and vomiting (P = 0.019), pain (P = 0.002), dyspnea (P < 0.001), appetite loss (P = 0.007), and diarrhea (P = 0.004) (Fig. 4). Worse QoL, as evidenced by generally lower individual domain scores, was seen for patients with NSCLC, gastric tumors, and HN tumors, and worse symptoms, as evidenced by generally higher individual symptom scores, were seen for patients with gastric tumors and RCC.
Fig. 4
Mean (SD) post-recurrence EORTC QLQ-C30 symptom scores for all patients, by tumor type, and by type of recurrence. a Wilcoxon rank sum test. DM distant/metastatic, EORTC QLQ-C30 European Organisation for Research and Treatment of Cancer Core Quality of Life questionnaire, HN head and neck, LR locoregional recurrence, NSCLC non-small cell lung cancer, RCC renal cell carcinoma, SD standard deviation, TNBC triple-negative breast cancer
When EORTC QLQ-C30 outcomes were evaluated by type of recurrence, global health status/QoL was significantly worse (P < 0.001) for patients with a distant/metastatic recurrence versus a locoregional recurrence (Figs. 3 and 4). When individual domain scores were analyzed, patients with a distant/metastatic recurrence had significantly more impairment than those with a locoregional recurrence as demonstrated by lower mean (SD) scores in the physical functioning (54.5 [34.1] vs 67.8 [27.4], P = 0.018), emotional functioning (39.9 [31.2] vs 55.0 [26.6], P = 0.001), cognitive functioning (47.8 [31.5] vs 67.8 [28.8], P < 0.001), and social functioning (40.1 [37.8] vs 55.9 [32.4], P = 0.007) domains (Fig. 3). Compared with patients with locoregional recurrence, patients with distant/metastatic recurrence experienced more financial difficulties, as demonstrated by their higher mean (SD) scores (62.2 [41.2] vs 45.1 [37.1], P = 0.006). They also experienced greater symptomatology, as evidenced by their higher mean (SD) scores across these symptoms: fatigue (65.8 [32.7] vs 53.0 [28.7], P = 0.009), nausea and vomiting (34.3 [31.2] vs 20.2 [24.6], P = 0.005), pain (60.3 [37.7] vs 48.0 [30.9], P = 0.031), dyspnea (47.4 [39.2] vs 30.2 [28.5], P = 0.007), insomnia (67.3 [34.6] vs 48.2 [28.5], P < 0.001), and appetite loss (54.5 [40.2] vs 34.7 [35.8], P = 0.002) (Fig. 4).
De Novo QoL QuestionsPost-recurrence, many patients reported worrying “quite a bit” or “very much” about their cancer getting worse or coming back (76.2%), feeling a loss of hope or feeling hopeless (40.0%), feeling anxious (56.4%), and feeling stressed about their condition (59.9%) (Fig. 5). Significant differences in responses were seen across tumor types for the questions “Have you felt anxious?” (P = 0.007) and “Have you felt stressed about your condition?” (P = 0.039), with the greatest proportions of patients selecting the “very much” response to these two questions having gastric cancer (52.6% and 52.6%) or NSCLC (40.0% and 40.0%).
Fig. 5
Patient QoL pre-recurrence and post-recurrence by tumor type and type of recurrence as measured by de novo questions. aResults post-recurrence differed statistically between those with a locoregional and distant/metastatic recurrence (P = 0.074). bResults post-recurrence differed statistically between those with a locoregional and distant/metastatic recurrence (P < 0.001). cResults post-recurrence differed statistically across tumor types (P = 0.007) and between those with a locoregional and distant/metastatic recurrence (P = 0.012). dResults post-recurrence differed statistically across tumor types (P = 0.039) and between those with a locoregional and distant/metastatic recurrence (P = 0.006). DM distant/metastatic, HN head and neck, LR locoregional recurrence, NSCLC non-small cell lung cancer, QoL quality of life, RCC renal cell carcinoma, TNBC triple-negative breast cancer
The analysis by type of recurrence also found that many patients with a locoregional or distant/metastatic recurrence reported worrying “quite a bit” or “very much” about their cancer getting worse or coming back (73.4% and 84.7%), feeling any loss of hope or feeling hopeless (34.6% and 57.7%), feeling anxious (52.7% and 67.3%), and feeling stressed (56.7% and 69.2%) post-recurrence (Fig. 5). Post-recurrence, significant differences between patients with a distant/metastatic recurrence compared with a locoregional recurrence were seen for the questions evaluating loss of hope (P < 0.001), anxiety (P = 0.012), and stress (P < 0.006). For all three of these questions, a greater proportion of patients with a distant/metastatic than locoregional recurrence selected “very much” and a smaller proportion “not at all.”
From pre-recurrence to post-recurrence for all patients, the proportion selecting “quite a bit” or “very much” compared with “not at all” or “a little” increased when patients were asked if they worried about their cancer getting worse or coming back, felt a loss of hope or felt hopeless, felt anxious, or felt stressed (Fig. 5). Results were similar when evaluated by type of recurrence and tumor type.
Caregiver SurveyEQ-5D-5LPost-recurrence, the mean (SD) EQ-5D-5L index score was 0.84 (0.16) and VAS score was 81.2 (13.4) for caregivers (Fig. 6). Across the different tumor types, no significant differences were seen for caregivers, with mean (SD) index scores post-recurrence ranging from a low of 0.76 (0.18) among caregivers of those with RCC to a high of 0.87 (0.14) among caregivers of those with NSCLC and 0.87 (0.11) among those with melanoma. Significant differences were seen in VAS scores across caregivers of patients with different tumor types post-recurrence (P = 0.005), with the worst QoL as signaled by VAS scores reported by caregivers of those with RCC (72.0 [8.8]) and HN tumors (73.4 [15.3]).
Fig. 6
Mean (SD) caregiver post-recurrence EQ-5D-5L index and VAS scores by tumor type and type of recurrence. a Wilcoxon rank sum test. DM distant/metastatic, HN head and neck, LR locoregional recurrence, NSCLC non-small cell lung cancer, RCC renal cell carcinoma, SD standard deviation, TNBC triple-negative breast cancer, VAS visual analog scale
The analyses by type of recurrence found that post-recurrence, QoL was worse in caregivers of people with a distant/metastatic compared with a locoregional recurrence as seen in lower mean (SD) index (0.78 [0.19] vs 0.86 [0.15], P = 0.23) and VAS scores (75.5 [16.4] vs 83.5 [11.2], P = 0.022) (Fig. 6).
Information on the EQ-5D-5L individual domain health states for caregivers can be found in Sect. 2.2.1 of the electronic supplementary materials and Fig. S2.
CarGOQoLThe mean CarGOQoL score across all caregivers was 62.0 (18.3) and did not differ significantly across tumor types post-recurrence (Fig. 7). The lowest QoL, as signaled by the lowest CarGOQoL scores, was reported by caregivers of people with RCC (55.5 [18.5)] and HN tumors (55.9 [19.6]).
Fig. 7
Change in mean (SD) CarGOQoL global scores from pre-recurrence to post-recurrence by tumor type and type of recurrence. aUnequal t test. bEqual t test. c Wilcoxon rank sum test. dMean global CarGOQoL scores differed significantly between caregivers of people with a distant/metastatic vs locoregional recurrence, P = 0.016. CarGOQoL CareGiver Oncology Quality of Life questionnaire, HN head and neck, NSCLC non-small cell lung cancer, RCC renal cell carcinoma, SD standard deviation, TNBC triple-negative breast cancer
Mean CarGOQoL scores post-recurrence differed significantly according to the type of recurrence, with caregivers of people with a distant/metastatic recurrence showing worse QoL as measured by the CarGOQoL global score compared with caregivers of people with a locoregional recurrence (54.9 [19.6] vs 64.8 [17.0], P = 0.016) (Fig. 7).
From pre-recurrence to post-recurrence, a deterioration in QoL was seen for all caregivers, with mean (SD) global CarGOQoL scores significantly decreasing from 73.1 (12.2) to 62.0 (18.3) (P < 0.001) (Fig. 7). When results were evaluated by tumor type, significant decreases in mean (SD) global CarGOQoL scores from pre-recurrence to post-recurrence were seen in caregivers of those with melanoma (79.5 [8.9] vs 67.4 [16.0], P = 0.016), RCC (71.1 [11.7] vs 55.5 [18.5], P = 0.029), and gastric tumors (68.0 [8.9] vs 57.5 [13.2], P = 0.032).
Information on the CarGOQoL individual domain scores across tumor types, by type of recurrence, and from pre-recurrence to post-recurrence can be found in Sect. 2.2.2 of the electronic supplementary results and Fig. S3.
De Novo QoL QuestionsWhen caregivers were asked post-recurrence if they worried about the cared-for person’s cancer getting worse or coming back, 19.0% selected “sometimes-moderately,” 25.0% “often-a lot,” and 44.0% “always-enormously”; no significant differences were seen across tumor types (Fig. S4). When asked if caring for the person was challenging post-recurrence, 36.0% of caregivers selected “sometimes-moderately,” 22.0% “often-a lot,” and 11.0% “always-enormously,” with no differences identified across tumor types.
Additional information on the de novo QoL questions by type of recurrence and from pre-recurrence to post-recurrence can be found in Sect. 2.2.3 of the electronic supplementary results and Fig. S4.
Comments (0)