
Remember me


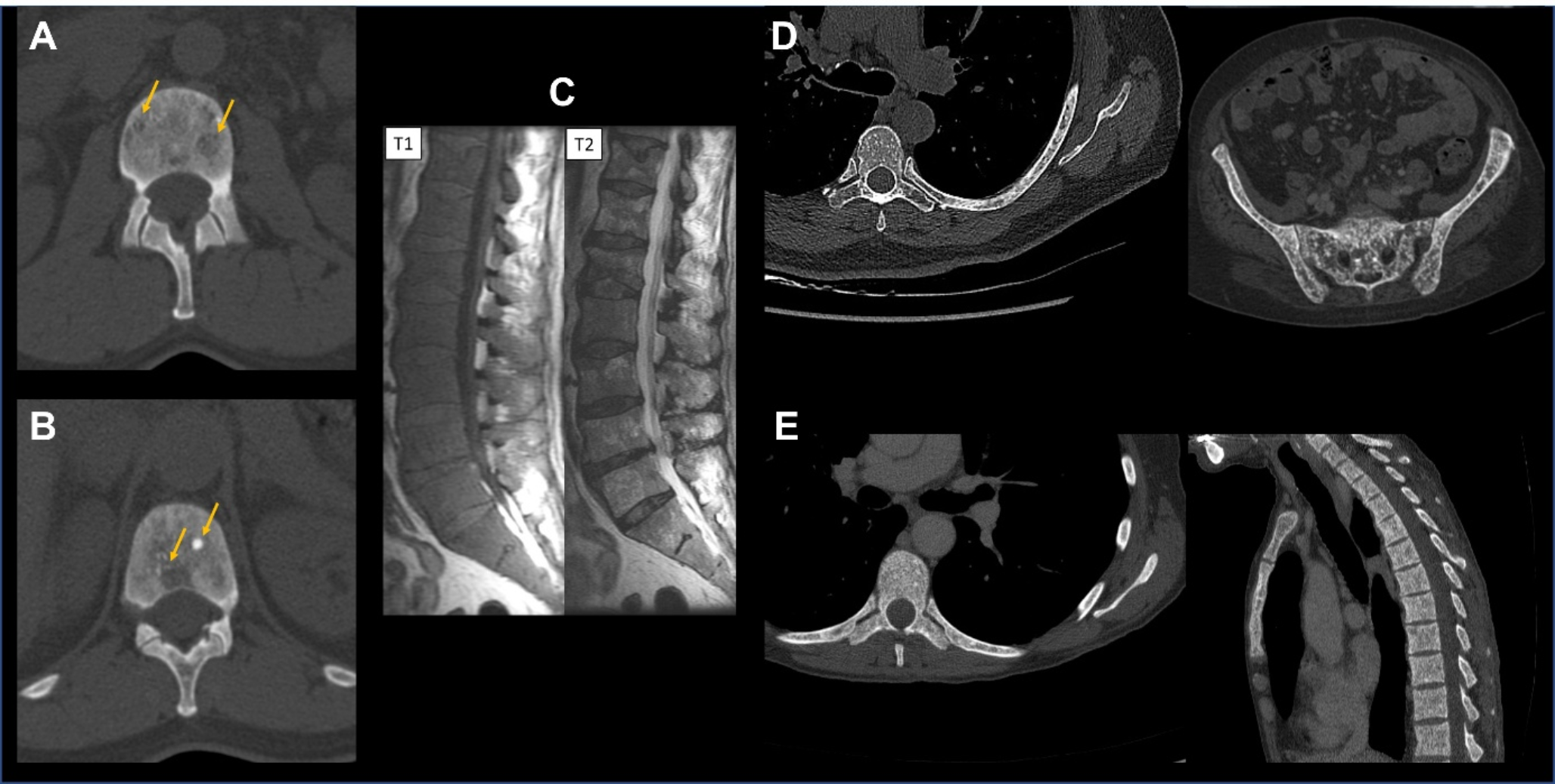
Bone involvement in systemic mastocytosis is highly heterogeneous. It can include: radiological findings (Fig. 1) such as diffuse bone resorption referred to as osteoporosis; focal bone resorption referred to as osteolysis; diffuse bone condensation referred to as osteosclerosis; focal bone condensation; and bone marrow infiltrate [4, 5]. Mixed patterns are common. Thorough analysis of bone lesions is important, as they serve as prognostic markers. Large osteolytic lesions (i.e., > 2 cm), diffuse osteosclerosis and bone marrow infiltrate (hypointense T1W, hyperintense T2W and STIR signal in MRI) are patterns observed in advanced SM, whereas osteoporosis, small osteolytic lesions and focal bone condensation are usually observed in non-advanced SM [6].
Fig. 1
Main bone radiological involvement in systemic mastocytosis. (A) Spine CT-scan with vertebral focal osteolytic lesions. (B) Spine CT-scan with mixed lesions on the same vertebra with both focal osteolysis and focal osteocondensation. (C) Spine MRI with diffuse infiltration consisting of hypointense signal in T1-weighted sequence and heterogeneous T2 signal in fat-saturated sequence. (D) Spine and pelvis CT-scan with disseminated punctiform osteocondensations. (E) Spine CT-scan with diffuse bone marrow sclerosis/osteosclerosis
In addition, patients often report bone pain, with this non-specific manifestation occurring in 10 to 31% of cases [7,8,9]. This assessment remains a challenge since it requires medical expertise in musculoskeletal pathologies (often by the rheumatologist) to rule out differential and/or associated diagnoses, including common conditions such as osteoarthritis, common low back pain and fibromyalgia.
Pathophysiology of Osteoporosis in MastocytosisTwo histomorphometry studies have described the bone remodeling abnormalities in SM [10, 11]. SM is associated with a moderate bone hyper-resorption, characterized by an increase in the number and activity of osteoclasts [10, 11]. The resorption lacunae are not in direct contact with the mast cell nodules [10]. In parallel, osteoblastic formation is similar to that of osteoporotic patients without mastocytosis, with mast cells adjacent to osteoblasts or lining cells. VCAM-1 adhesion protein expressed by mast cells is thought to enable their adhesion onto osteoblasts/lining cells expressing α4β7 or α4β1 integrins [10]. There are also mineralization abnormalities, with a significant increase in the bone formation rate (BFR/BV ratio) [10]. Mast cells are thought to influence bone cells through the secretion of heparin, histamine, tryptase, IL-1, and IL-6 [12,13,14,15]. In addition, a more recent study has identified micro-RNA (miR-23a and miR-30a) contained in mast-cell-derived extracellular vesicles as potential new players of this pathogeny [16].
Epidemiological Considerations for OsteoporosisAmong all forms of mastocytosis, indolent SM (ISM) has historically been considered as associated with bone involvement and osteoporosis [17, 18]. SM prevalence in Europe is estimated at 1/1000 to 1/10,000. However, this value is probably largely underestimated due to the non-specific nature of its symptoms and a lack of awareness of the disease on the part of both practitioners and the general public. Single-center data from a German study showed that with systematic bone biopsy in 1374 patients referred for osteoporosis, the prevalence of indolent SM was 0.5%, and even > 5% in young men with osteoporosis [19].
Osteoporosis is a classical manifestation of SM, affecting up to 30% of patients, including young males (who are not commonly affected by osteoporosis), and it is responsible for a specific spine osteoporosis and multiple vertebral fractures [7, 20,21,22,23,24,25].
Among SM forms, bone marrow mastocytosis (BMM) is now individualized from ISM, and is characterized by the absence of skin lesions and B-findings and a basal serum tryptase below 125 ng/ml [26, 27]. BMM is frequently observed in rheumatological practice and does not differ from ISM in terms of bone presentation. In our expert center, BMM represents ~ 17% of all cases of non-advanced systemic mastocytosis (including smoldering systemic mastocytosis) [21].
Other forms of mast cell diseases may be associated with bone involvement and especially osteoporosis. Recent data highlight the high frequency of osteoporosis in monoclonal mast cell activation syndrome (MMAS) [21, 28]. However, its presentation seems to differ from that of ISM and BMM, with frequent additional explanatory risk factors for osteoporosis and fewer vertebral fracture cascades [21].
Tools to Assess Bone HealthBone involvement can be readily assessed in routine care. Biological assessment relies on measuring the markers of bone metabolism. These includes (but are not limited to) serum calcium and phosphorus, 25OH vitamin D, alkaline phosphatase, and serum C-telopeptides of collagen type 1 (serum crosslaps or CTX, as biomarker of bone resorption). Radiological assessment involves measuring bone mineral density (BMD) by dual x-ray absorptiometry (DXA), X-rays, CT-scan and MRI. Methods of bone health assessment are recalled in Table 1.
Table 1 Routine methods of bone health assessment in mastocytosis. ALP: alkaline phosphatase; DXA: dual x-ray absorptiometry; GFR: glomerular filtration rate; MRI: magnetic resonance imaging; PET-scan: Positron emission tomography; SD: standard deviation; WHO: World Health OrganizationX-ray evaluation of thoraco-lumbar spine should be performed in routine to assess the presence of radiographic fractures. CT-scan is useful as second line, and helps to better identify the bone structural abnormalities (osteocondensation, osteoresorption). MRI should not be systematic. MRI appears relevant in case of back pain to confirm recent vertebral fracture (bone marrow oedema of the fractured vertebra), and in case of suspected advanced systemic mastocytosis to evaluate medullar involvement and possible large osteolytic lesions. Given the performance of MRI, bone scintigraphy as a limited usefulness, and may be used as second line (in case of unavailable MRI) to identify recent fractures. These fractures being associated with vertebral hyperfixation of the radiotracer (usually technetium-99 m). To date, PET-CT is not recommended as a routine exam to assess bone health in SM. Its diagnostic value, its prognostic value, and its incremental value (in addition to X-ray/CT and MRI) need further evaluation for bone disease in SM.
Assessment of Osteoporosis Risk in MastocytosisClinical Assessment of OsteoporosisTrabecular osteoporosis with multiple vertebral fractures is a major hallmark of SM. Clinicians managing these patients have to identify bone fragility and its risk factors. Bone fragility must be mentioned in case of a history of low-energy fracture, defined by a fracture occurred during a fall from one’s height, while walking and obviously when occurring spontaneously.
Special attention should be paid to vertebral fractures, which in one third of cases are asymptomatic. In this case, a loss of stature of 2 cm compared to the previous measurement or 4 cm compared to the historical size indicate a potential vertebral fracture of fractures and therefore should lead to spinal X-ray imaging.
The evaluation of risk factors for osteoporotic fractures largely relies on the usual screening process proposed for postmenopausal osteoporosis [29, 30]. These include risk of fall, glucocorticoid use, early menopause, low body mass index (< 19), alcoholism and smoking.
DXA ScreeningDXA scan is essential for the assessment of bone strength (Table 1). This exam identifies patients with low BMD defined as a T-score ≤-2.5 SD in postmenopausal women and males > 50 years old. On the contrary to post-menopausal osteoporosis, the threshold for osteoporosis definition in young adults is not consensual. In young adults, osteoporosis is often defined as a Z-score <-2 SD.
Importantly, the DXA is above the threshold of osteoporosis definition in one third of cases of patients with genuinely osteoporotic fractures. A patient with fragility fractures, but a T-score > -2.5 SD should be considered as osteoporotic in most cases [31]. This discrepancy is commonly observed in all forms of osteoporosis, including steroid-induced and postmenopausal, because some of the parameters of bone strength are not evaluated by DXA.
In addition, the presence of vertebral fractures, of osteoarthritis, of surgical equipment or of any situation that artefactually increases BMD in the region of interest generates an overestimation of BMD and subsequently false negatives for DXA-based osteoporosis screening.
Regarding DXA-screening repetition: a close annual follow-up may be considered for SM patients with osteoporosis, especially in severe osteoporosis (with fractures). However, it appears that for SM patients without osteoporosis at the initial assessment, a re-evaluation with bone densitometry within 2 years may not be necessary if the initial crosslaps levels are low [32].
Prediction of Fracture OccurrenceTo date, the validated predictors associated with the occurrence of vertebral fractures in SM are: low hip T-score; age at diagnosis; and male gender [24, 31]. The level of bone marrow tryptase is also potentially associated with the osteoporotic fracture phenotype in SM; however, this biomarker needs validation in independent cohorts [31, 33]. The value of crosslaps has also been studied. The association between serum crosslaps and osteoporotic fracture phenotype is still the subject of debate [24, 34].
Surprisingly, current covariates proposed to explain OP in ISM are non-specific for ISM. No biomarker specific for ISM is currently used in common medical practice to stratify OP risk in ISM. Serum IL-6 and IL-1β levels may be of interest, but are not used in daily practice [13,14,15, 35].
From the perspective of prediction, the MastFx score was proposed in 2014 as a means of distinguishing between patients with a high, intermediate or low osteoporotic fracture risk among patients with ISM [24]. This score considers the presence of five items identified at diagnosis: male sex; serum CTX (Z-score of CTX > + 1 SD); bone mineral density of the hip (T score <-1 SD); absence of urticaria pigmentosa; and alcohol consumption. This score needs validation in independent cohorts.
Situations in Which Mastocytosis-Related Osteoporosis is SuspectedThe following situations are suggestive of mastocytosis-related osteoporosis:
Vertebral osteoporosis in young males < 40–50 years old;
Vertebral osteoporosis with cutaneous or “allergic” signs;
Vertebral osteoporosis not responding to conventional anti-osteoporotic treatments;
Vertebral fracture cascade in a subject who is not at risk of osteoporosis.
In these situations, SM needs to be ruled out at diagnosis. A thorough skin examination is needed. A first screening step may consist of measuring serum tryptase and searching for KIT mutations in blood by ASO-qPCR or digital PCR, if available [36, 37].
Treatment of OsteoporosisPoints to Consider Before Treating Mastocytosis OsteoporosisBefore treating mastocytosis osteoporosis, clinicians first need to determine whether SM is the only contributor to osteoporosis. If not, management of (i) the associated conditions for secondary osteoporosis (e.g., primary hyperparathyroidism, glucocorticoid use, alcoholism,) or of (ii) postmenopausal status (which represents the main etiology for osteoporosis) is required. To date, no validated biomarker is available to estimate the contribution of SM in osteoporosis when additional causes are associated. Bone marrow tryptase measurement may be a promising biomarker, but still needs to be validated for use in such contexts [20].
Secondly, the presence of vertebral fractures needs to be considered. This feature indicates a severe osteoporosis (according to the WHO definition [29]) and should lead to a more intensive treatment compared to densitometric osteoporosis (i.e., T-score ≤-2.5 without fragility fracture).
Fall risk must also be considered. Falls are markers of frailty and strongly influence the likelihood of fragility fractures. Even though falls are less critical than in non-vertebral fractures, fall risk assessment still has its uses. This assessment includes identification of: (i) risk conditions (balance disorders, sarcopenia, vision disorders, sedative and/or hypotensive medication, cognitive disorders and vitamin D deficiency); (ii) one or several falls during the past year; and (iii) simple dedicated tests in patients without a history of falls (get-up-and-go test, single-leg stance test, sternal nudge test).
The last point to consider is the patient’s metabolic and hormonal status with respect to bone health: ~1000 mg daily calcium dietary intake and sufficient vitamin D intake to reach 25(OH) vitamin D level ≥ 30 ng/ml are recommended in postmenopausal osteoporosis, and should be in osteoporosis of SM.
Efficacy of Anti-Osteoporotic Drugs in MastocytosisBone-modifying agents such as bisphosphonates represent the historical cornerstone for osteoporosis treatment in SM [38]. However, this practice is based on expert recommendation without randomized studies to prove their efficacy in SM [2, 7, 39,40,41]. The limited amount of published research only studies low numbers of patients and contains discrepancies in terms of treatment regimen and, in some cases, insufficient levels of reported data regarding bone assessment, thus explaining the low level of evidence. Importantly, the severity of osteoporosis (i.e., with fragility fracture), the type of bisphosphonate used and the rate of incident fractures during follow-up, although fundamental elements, are often not reported. In densitometric osteoporosis (without fracture), either oral bisphosphonates or intravenous (iv) bisphosphonates (zoledronic acid and pamidronate) seem to represent a relevant option (Table 2). Conversely, in cases of severe osteoporosis, fracture risk is only partially mitigated by bisphosphonates and oral bisphosphonate are insufficient; iv bisphosphonates or other treatments should be considered [40, 42].
Table 2 Anti-osteoporotic therapies in indolent systemic mastocytosis. BMD: bone mineral density; DXA: dual x-ray absorptiometry; ISM: indolent systemic mastocytosis; IFN: interferon; IV: intravenous; n.a.: not available TIW: three times a weekDenosumab, a monoclonal antibody against the receptor activator of nuclear factor κ B ligand (RANKL), is a potent antiresorptive agent and is approved for postmenopausal and male osteoporosis with high risk of fractures. This drug has been assessed in SM [43]. Despite promising densitometric results, questions remain about both its efficacy in reducing fractures and its tolerance. Importantly, the biological effect of denosumab is associated with a transient (i.e., limited to drug exposition period) and robust inhibition of bone turnover markers [44]. This inhibition of bone turnover markers goes alongside an inhibition of bone resorption reflected by reduced eroded surface and a gain in BMD [44]. However, denosumab withdrawal is associated with a “rebound phenomenon” characterized by: (i) an increase in bone turnover marker levels usually within the first six months following the cessation of treatment; (ii) a decrease in BMD; and (iii) an unexpected increased risk of (multiple) vertebral fractures [45]. Given the propensity of the SM patients to develop vertebral fractures, this rebound phenomenon may be exacerbated after being treated with denosumab and therefore needs careful evaluation and management. Answers would probably be provided by the results of the DenosuMast study (NCT03401060), which evaluates the densitometric (BMD) efficacy of 60 mg of denosumab every six months versus placebo over three years in patients with SM.
Teriparatide, a bone anabolic recombinant peptide derived from intact human parathyroid hormone, is validated for osteoporosis treatment. This drug is of particular interest in patients with predominant vertebral osteoporosis and vertebral fractures. However, to our knowledge, there is currently no probative report of its anti-fracture efficacy in SM. In addition, in our expert center experience, some patients with severe osteoporosis were referred because of teriparatide inefficacy leading finally to the diagnosis of SM [42]. Its place in the management of osteoporosis in SM needs thorough assessment.
Efficacy of Mastocytosis Treatment on OsteoporosisWhereas first line treatment of osteoporosis is usually bisphosphonates, the usual approach to treat secondary osteoporosis is to treat the underlying condition, so as to improve bone strength. As such, interferon, a treatment for SM has been historically proposed to treat osteoporosis in SM. In severe osteoporosis, SM-specific treatments should be considered (Table 2). Here too, supporting studies are limited to case series and small cohorts [42, 46,47,48,49]. Importantly, only one study specifically evaluated this challenging situation and reported a positive long-term impact of the combination of interferon (IFN) and pamidronate, with a very high increase in BMD and a low re-fracture rate [47]. Other molecules, such as midostaurin and masitinib, did not demonstrate such efficacy [42].
To date, combining the transient specific effect of IFN with the long-lasting effect of pamidronate seems to be the strategy with the best level of evidence in cases of severe osteoporosis [47]. However, IFN tolerance is often poor. There is no available evidence about mast cell blockers, such as antihistamine, in treating osteoporosis in SM.
Proposal for Osteoporosis TreatmentBased on the available data and on our expert center experience, we propose the following strategy for the treatment of osteoporosis in SM.
To treat densitometric osteoporosis (T-score ≤ -2.5 SD without fracture), the first-line treatment involves bisphosphonates. Options include yearly IV (intravenous) zoledronic acid (5 mg), weekly alendronate, or weekly risedronate. For second-line treatment, denosumab or switching between different bisphosphonates should be considered.
In the case of severe osteoporosis with vertebral fractures, the first-line treatment consists of intensive therapy during the first year, including monthly IV pamidronate, potentially combined with weekly peginterferon alfa-2a, followed by quarterly IV pamidronate for another year. Peginterferon alfa-2a should be considered if there are multiple vertebral fractures. If there is intolerance to either interferon or pamidronate, dose reduction may be considered. For second-line treatment, options include quarterly IV zoledronic acid (4 mg) and specific treatments for mastocytosis, such as a new tyrosine kinase inhibitor (ITK). However, the evidence for these alternatives is currently limited.
Treatment of Bone PainRuling Out Differential DiagnosisOsteoporosis management in SM is often successful. Bone pain management, however, remains difficult due to the lack of a validated treatment. When dealing with a patient with bone pain, the critical first step is to identify its origin. The available studies do not tend to report whether differential diagnosis has been appropriately ruled out. This may explain the important variability in the rate of bone pain across studies. In our expert center experience, common diagnoses, such as osteoarthritis, common low back pain or fibromyalgia, are often the cause of bone pain. In most cases, a proper rheumatological/musculoskeletal examination and first-line examinations, such as X-rays and ultrasounds of painful areas, are sufficient to clarify the etiology when SM-independent.
Symptomatic TreatmentsBone pain is thought to be partly related to mast cell degranulation [
Comments (0)