
Remember me


Although bariatric surgery can result in significant weight loss and numerous health benefits [4], surgical weight loss is increasingly recognized to adversely affect bone metabolism [5]. The extent of high-turnover bone loss suggests severe bone impairment, and this phenomenon is larger than that observed in weight loss related to calorie restriction [5]. This is likely related, at least in part, to the magnitude of weight loss after bariatric surgery. The changes in bone turnover markers (BTMs) and bone mineral density (BMD) are similar to those found in calorie restriction: serum collagen type I cross-linked C telopeptide (CTX) levels increase to a greater extent than those of procollagen type I N-propeptide (PINP), and total hip BMD decreases to a greater extent than lumbar spine BMD [6, 7]. After Roux-en-Y gastric bypass (RYGB), PwO also experiences substantial deterioration in bone microarchitecture and strength, as assessed using high-resolution peripheral quantitative computed tomography (HR-pQCT) [8, 9].
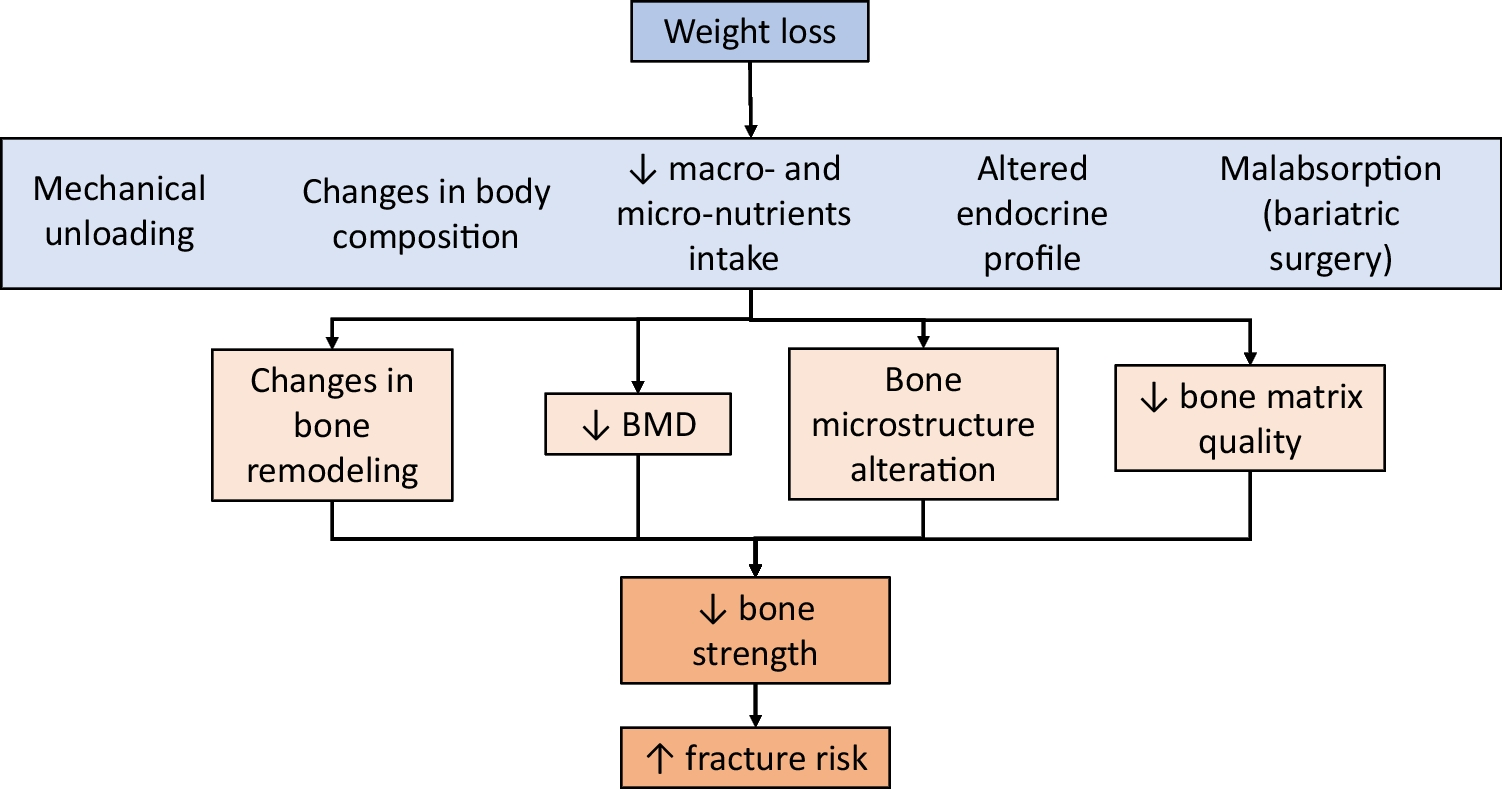
Undoubtedly, there is an association between surgical weight loss and a higher risk of fracture, which usually emerges in the 3rd year of follow-up [10, 11]. Although the underlying mechanisms are not fully understood, many factors are involved, including nutritional factors, mechanical unloading, loss of muscle mass, changes in the secretion of gut hormones and adipokines, and an increased risk of falls (Fig. 1) [5, 12]. Accumulating evidence suggests that RYGB is associated with a greater reduction in BMD, greater increase in BTMs, and higher risk of fragility fractures than sleeve gastrectomy (SG) [5, 10]. In addition, postmenopausal women are at highest risk for skeletal consequences than premenopausal women and men.
Fig. 1
Mechanisms of bone loss associated with intentional weight loss, (adapted from Papageorgiou M & Biver E. Rev Med Suisse. 2023 Apr 19;19(823):756–760)
Management of Adverse Skeletal Effects Following Bariatric SurgeryThe American Society for Metabolic and Bariatric Surgery (ASMBS) released its initial position statement in 2015, with an update in 2020 [13]. Furthermore, guidelines for preventing and treating osteoporosis resulting from bariatric surgery were provided in 2022 by the European Calcified Tissue Society (ECTS) [14] and the joint efforts of the Osteoporosis Research and Information Group (GRIO) and French Rheumatology Society (SFR) [15]. A summary of these recommendations is provided in Table 1.
Table 1 Summary of the main guidelines on the prevention and treatment of osteoporosis secondary to bariatric surgeryScreeningFor patients aged 50 years and older, including post-menopausal women, the evaluation should include clinical risk factors including a fracture history, alcohol consumption, and smoking habits, DXA testing of the lumbar spine and hip, spine radiographs or vertebral fracture assessment, measurement of BTMs, and biochemical analyses to identify secondary causes of osteoporosis. This assessment should ideally be performed before any bariatric surgery, regardless of the specific procedure [14, 15]. Some guidelines suggest that all patients undergoing RYGB and biliopancreatic diversion with duodenal switch (BPD/DS) should have their BMD and clinical risk factors evaluated due to the substantial bone loss and elevated fracture risk associated with these malabsorptive procedures [15]. Moreover, patients considered at high risk should undergo these evaluations, regardless of age. High-risk status is determined by either experiencing a fragility fracture after age 40 years, having comorbidities, or taking medications linked to osteoporosis (e.g., corticosteroids, aromatase inhibitors) [15].
A study by Blom-Høgestøl et al. investigated the occurrence of osteopenia, osteoporosis, and fragility fractures in 124 patients a decade after undergoing RYGB [16]. The study population had a mean age of 50.3 years (standard deviation (SD) 9.0), with 77% (n = 94) being female, of whom 44% (n = 41) were postmenopausal. Among the 59 participants who were postmenopausal women or men aged 50 years or older, osteopenia was found in 51% (n = 30) and osteoporosis in 27% (n = 16). This study did not provide information on the prevalence of BMD T-scores ≤ − 2. Fragility fractures were also common in this group. Nineteen percent (n = 11) of postmenopausal women and men aged 50 years or above reported having experienced a fragility fracture. DXA scans for vertebral fracture assessment revealed that 8% (n = 5) of the participants had at least one moderate or severe morphometric vertebral fracture [16].
A retrospective cohort study assessed the application of the ECTS guidelines in postmenopausal women and men aged ≥ 50 years who had undergone bariatric surgery [17]. This study, conducted from February 2019 to March 2022, included 170 patients (144 females; median age, 59 [55–63] years). The results showed that 33 patients qualified for anti-osteoporosis medication (AOM), indicating a prevalence of 19.6% [CI 95%: 13.9%–26.5%]. Most of these patients met the criteria based on a BMD T-score of −2 or lower (n = 25, 14.7% [CI 95%: 9.7%–20.9%]) and/or a recent history of fragility fractures (n = 12, 7.1% [CI 95%: 3.7%–12.0%]) [17]. This study was the first to evaluate the applicability and usefulness of the ECTS guidelines; however, the findings need to be confirmed to better determine the targeted population for evaluation and AOM in the context of surgical weight loss.
Non-pharmacological MeasuresSeveral studies have highlighted the positive effects of lifestyle changes in preventing bone loss; however, data on fracture outcomes are currently unavailable. It is generally accepted that following bariatric procedures, sufficient intake of calcium, vitamin D, and protein, along with regular exercise, is crucial to counteract the negative effects on the bone and muscle [5, 12].
Exercise TrainingThe BABS study, an interventional study, demonstrated a positive effect on BMD and BTMs through combined supplementation of vitamin D, calcium, and protein powder (35–60 g/day), coupled with aerobic exercise (Nordic walking, strength perseverance, and equipment training) [18] (Supplementary Table 1). The intervention group experienced a smaller decrease in total hip BMD (−3.9% vs. −9.9%, p < 0.001) and a smaller increase in BTMs (82.6% vs. 158.3%, p < 0.001 for CTX and 12.0% vs. 41.2%, p = 0.003 for PINP) than the control group. Three studies confirmed that a supervised exercise regimen consisting of weight-bearing and aerobic activities mitigated the reduction in BMD and BTMs typically observed following surgical weight loss [19,20,21]. In another study involving 154 patients, no treatment effect of exercise training was observed at 12 months on BMD, submitted to (single anastomosis, Roux-en-Y) gastric bypass, or SG. However, the exercise training duration was short [12 weeks], with only 1 session per week [22] (Supplementary Table 1).
Overall, studies have shown a lower decrease in BMD after an exercise training program, including both aerobic and resistance training. French guidelines suggest that aerobic and strength exercise programs alongside nutritional interventions may be particularly advantageous for PwO patients who have undergone bariatric surgery and could help reduce long-term bone loss [15].
Vitamin D SupplementationCurrent recommendations exist for vitamin D supplementation before and after bariatric surgery [13,14,15, 23]. High-dose oral vitamin D3 supplementation (minimum 2,000 IU/day) is advised for PwO patients undergoing bariatric surgery, with intramuscular supplementation preferred over oral supplementation for those undergoing malabsorptive surgery [23]. A systematic review and meta-analysis provided data on vitamin D status and post-bariatric surgery vitamin D supplementation. The analysis included 39 studies with 5,296 patients [23]. Patients receiving high-dose oral vitamin D supplementation (≥ 2,000 IU/day, primarily the D3-formulation) showed lower rates of vitamin D insufficiency (25-hydroxyvitamin D (25(OH)D) < 30 ng/mL) and higher 25(OH)D levels post-surgery than those receiving low doses (< 2,000 IU/day), regardless of the type of procedure. For malabsorptive surgery, the prevalence of vitamin D insufficiency 6–24 months post-surgery was 43% versus 74% (p = 0.01), and 25(OH)D levels < 6 months postoperatively were 31 ng/mL versus 21 ng/mL (p = 0.03) [23].
Calcium IntakeDietary calcium intake is reduced owing to calorie restriction induced by bariatric surgery. Furthermore, after RYGB and SG, the digestive absorption of calcium was reduced [24, 25]. A prospective observational cohort study examined the effect of SG on intestinal fractional calcium absorption (FCA) in 35 severely obese individuals aged 24–70 years [25]. The assessment was conducted six months after surgery, with participants maintaining adequate 25(OH)D levels and consuming the recommended calcium intake of approximately 1200 mg daily. The results showed a significant decrease in mean (SD) FCA from 31.4 ± 15.4% before surgery to 16.1 ± 12.3% after surgery (p < 0.01) [25]. This finding indicates that RYGB is not the sole bariatric procedure associated with reduced intestinal FCA [24]. Therefore, calcium intake (dietary ± supplementation) should be at least 1200 mg/day after SG and 1500 mg/day after RYGB. Dietary intake should be preferred, that is, dairy products (low-fat if needed) and calcium-rich mineral water, but since this does not always cover the 1200–1500 mg/day requirement, medical supplementation is often needed to attain these levels [14, 15]. Although there are insufficient data in the literature to support a preference for one form of calcium supplementation over another (calcium citrate, calcium carbonate, or other), in the absence of gastric acidity, calcium citrate may be better absorbed. If secondary hyperparathyroidism persists despite reaching an optimal 25(OH)D concentration between 75 nmol/L (30 ng/ml) and 150 nmol/L (60 ng/ml), a deficiency in calcium intake that induces a negative calcium balance should be considered [14, 15].
Interestingly, a study involving 20 postmenopausal women who had undergone RYGB an average of five years earlier was conducted to evaluate the impact of prebiotics on intestinal FCA [26]. This randomized, double-blind, placebo-controlled trial administered either prebiotics or placebo orally for a 2-month period. Unfortunately, the results showed no significant differences between the groups in terms of changes in FCA or calciotropic hormones [26].
In summary, all PWO who are candidates for bariatric surgery or have already undergone bariatric surgery should follow these measures: ensure adequate calcium and protein intake, achieve a serum 25(OH)D concentration ≥ 30 ng/mL, mitigate fall risks, and engage in an appropriate physical activity regimen (Table 2).
Table 2 Non-pharmacological prevention and treatment of bone health impairment in all Bariatric Surgery-treated patientsPharmacological InterventionDetermining suitable standards for commencing AOM is crucial to address and prevent bone fragility caused by bariatric surgery. Various societies have differing views on the specific treatment criteria for postmenopausal women and men aged ≥ 50 years, based on the occurrence of fragility fractures and/or T-score thresholds [14, 15].
Most societies favor zoledronic acid (ZOL) as the primary option, because of issues with oral bisphosphonates intolerance and malabsorption [27]. Owing to safety reasons and the potential risk of anastomotic ulceration and direct gastric irritation, oral bisphosphonates should be avoided after bariatric surgery [27]. Denosumab is considered the secondary choice when bisphosphonates are contraindicated or not tolerated, owing to its associated risks, particularly the potential for rebound effects upon discontinuation [28, 29].
Information regarding the use of osteoanabolic agents for PwO after bariatric surgery is missing.
Nevertheless, the effectiveness of AOM in preventing bone loss following bariatric surgery remains partly unexplored, and there are currently no available data on fracture outcomes.
BisphosphonatesGiven the high-turnover bone loss state that occurs after bariatric surgery, it is logical to use inhibitors of bone resorption such as bisphosphonates.
Zoledronic AcidA small-scale, open-label pilot study conducted by Liu et al. over 24 weeks examined the initial safety and effectiveness of ZOL in suppressing BTMs and preventing BMD loss after RYGB. A single administration of ZOL before RYGB seemed to temporarily reduce, but not completely halt, the increased bone turnover. Furthermore, while ZOL might help maintain trabecular volumetric BMD (vBMD) in the spine (as measured by quantitative computed tomography (QCT)), it appeared inadequate in preventing bone loss at the total hip (as assessed by DXA) [30].
These findings were confirmed in a recent randomized, double-blind, placebo-controlled study conducted at a single public hospital in Denmark (the ZABAS study). Patients undergoing RYGB or SG were randomly assigned (1:1) to receive ZOL (5 mg) or placebo (PBO) preoperatively [31]. The primary endpoint was the change in lumbar spine vBMD at 12 months postoperatively, assessed using QCT. The secondary outcomes included changes in the hip and femoral neck BMD, aBMD, and bone turnover markers (CTX and PINP). The 59 patients (mean (SD) age: 49·6 ± 6·6, BMI: 42·3 ± 5·3, female/male: 42/17) were randomized to either received ZOL (n = 31) or PBO (n = 28). The estimated mean treatment effects of ZOL for the spine and total hip were 7.2 mg/cm3 (95% CI 2.5, 11.9, p = 0.003) and 5.4 mg/cm3 (95% CI 1.7, 8.9, p = 0.003), respectively. Areal BMD loss at the lumbar spine was prevented in the ZOL group (+ 1.4%), whereas the PBO group experienced a decline of −4.1%. Additionally, bone loss at the total hip was blunted for ZOL compared to PBO (vBMD: −1.6% vs. −4.9%, p = 0.003). Both groups experienced significant aBMD loss at the total hip compared to baseline, although the loss was larger in the PBO group than in the ZOL group (−4.0% vs. −8.0%, p < 0.0001). The C-terminal telopeptide of type I collagen increased in both groups but was lower in ZOL than in PBO (+ 101.0% vs. + 172.0%, p = 0.01) [31] (Supplementary Table 2). Serious adverse reactions were not observed. Flu-like symptoms were significantly higher in the ZOL group than in the PBO group (n = 18 vs. n = 6; p = 0.02). The prevalence of hypocalcemia did not differ between the groups [31].
Another pilot randomized controlled trial of ZOL (versus PBO) to prevent bone loss following SG is ongoing at the University of Nebraska (NCT04279392). This protocol was published in 2021 [32].
RisedronateThis (WE RISE) pilot study investigated the effectiveness of 150 mg of monthly oral risedronate in preventing bone loss associated with SG [33]. A group of 24 patients (mean (SD) age, 56 ± 7 years; 83% female, 21% black) was randomly assigned to receive either risedronate or a PBO for six months. This study measured changes in aBMD using DXA. After six months, significant differences were observed between the groups in the femoral neck (risedronate: + 1.3% vs. placebo: −4.2%) and lumbar spine (risedronate: + 2.2% vs. placebo: −2.2%) (both p ≤ 0.02). However, risedronate was not effective in halving the 6-month aBMD loss at the total hip (−2.6% versus −4.4%). No difference in PINP was noted between the groups (risedronate: 4% versus PBO: 4%), but the increase in CTX was significantly lower in the risedronate group (+ 68%) than in the PBO group (+ 175%) (p < 0.001). Initial treatment effect estimates suggest that 6 months of risedronate use may be effective in reducing aBMD loss in the lumbar spine after SG [33] (Supplementary Table 2). No serious adverse events (ulceration or hypocalcemia) were encountered by patients in this study [33].
Further data from a sufficiently powered trial are necessary for confirmation (STRONG BONES study, NCT04922333) [34].
DenosumabPreliminary results on the efficacy and safety of denosumab (DMAB) for preventing bone loss in individuals undergoing RYGB or SG were reported during the last American Society for Bone and Mineral Research (ASBMR) 2024 Congress in Toronto [35]. In a 2-site, double-blind, randomized placebo-controlled trial of 36 postmenopausal obese women and men aged > 50 years undergoing RYGB or SG, participants were randomized 2:1 to receive either DMAB 60 mg or placebo (PBO) every 6 months for 18 months beginning one month after surgery. Calcium citrate and vitamin D supplements were titrated to achieve and maintain a total calcium intake of 1500 mg/day and 25(OH)D level > 30 ng/mL. At the hip and spine, aBMD was measured using DXA at baseline and 7, 13, and 19 months postoperatively, and vBMD was measured using QCT at 1 and 19 months postoperatively. All 36 randomized participants (DMAB, n = 24; PBO, n = 12) completed the full 19-month trial. The DMAB and PBO groups were similar in age (57 ± 7 years), sex (67% female), baseline BMI (44 ± 6 kg/m2), and surgery type (72% SG). The DMAB and PBO groups lost similar amounts of weight (−24.6 ± 15 kg over 19 months). Participants with DMAB had increased aBMD and vBMD at all sites compared to those in the placebo group (Fig. 2). For total hip aBMD (primary endpoint), the mean (95% CI) between-group difference over 19 months was + 7.0% (+ 4.7%, + 9.4%) (p < 0.001), with mean within-group changes −6.4% for PBO and + 0.6% for DMAB. For spine aBMD, the between-group difference was + 8.4% (+ 3.7%, + 13.1%) (p < 0.001), with mean changes −4.1% for PBO and + 4.3% for DMAB. The between-group differences in vBMD were + 9.0%, + 8.7%, and + 9.5% for the total hip, femoral neck, and spine, respectively (all p ≤ 0.03). Six DMAB participants each experienced asymptomatic grade 1 hypocalcemia once (corrected calcium 8.0–8.4 mg/dL), while no hypocalcemia occurred with PBO (p = 0.08). There were no hypocalcemia grades 2–4 and no study-related serious adverse events in either group. In conclusion, denosumab may be an effective and safe option to prevent loss of bone mass in postmenopausal women and men aged > 50 years undergoing bariatric surgery [35]. The publication of these results is awaited. Furthermore, infusion with ZOL was planned 6 months after the 3rd injection of denosumab to avoid a rebound effect [35].
Fig. 2
Effects of denosumab (DMAB) versus placebo (PBO) at 7, 13, and 10 months on total hip and lumbar spine areal bone mineral density assessed by dual energy X-ray in individuals undergoing Roux-en-Y gastric bypass or Sleeve Gastrectomy
Comments (0)