Study Design and Patients
This was a retrospective, noninterventional, cohort study using data from three US claims datasets: Optum’s de-identified Clinformatics® Data Mart Database (Clinformatics®), Merative™ MarketScan® Commercial and Medicare Databases (MarketScan), and IQVIA US PharMetrics® (PharMetrics).
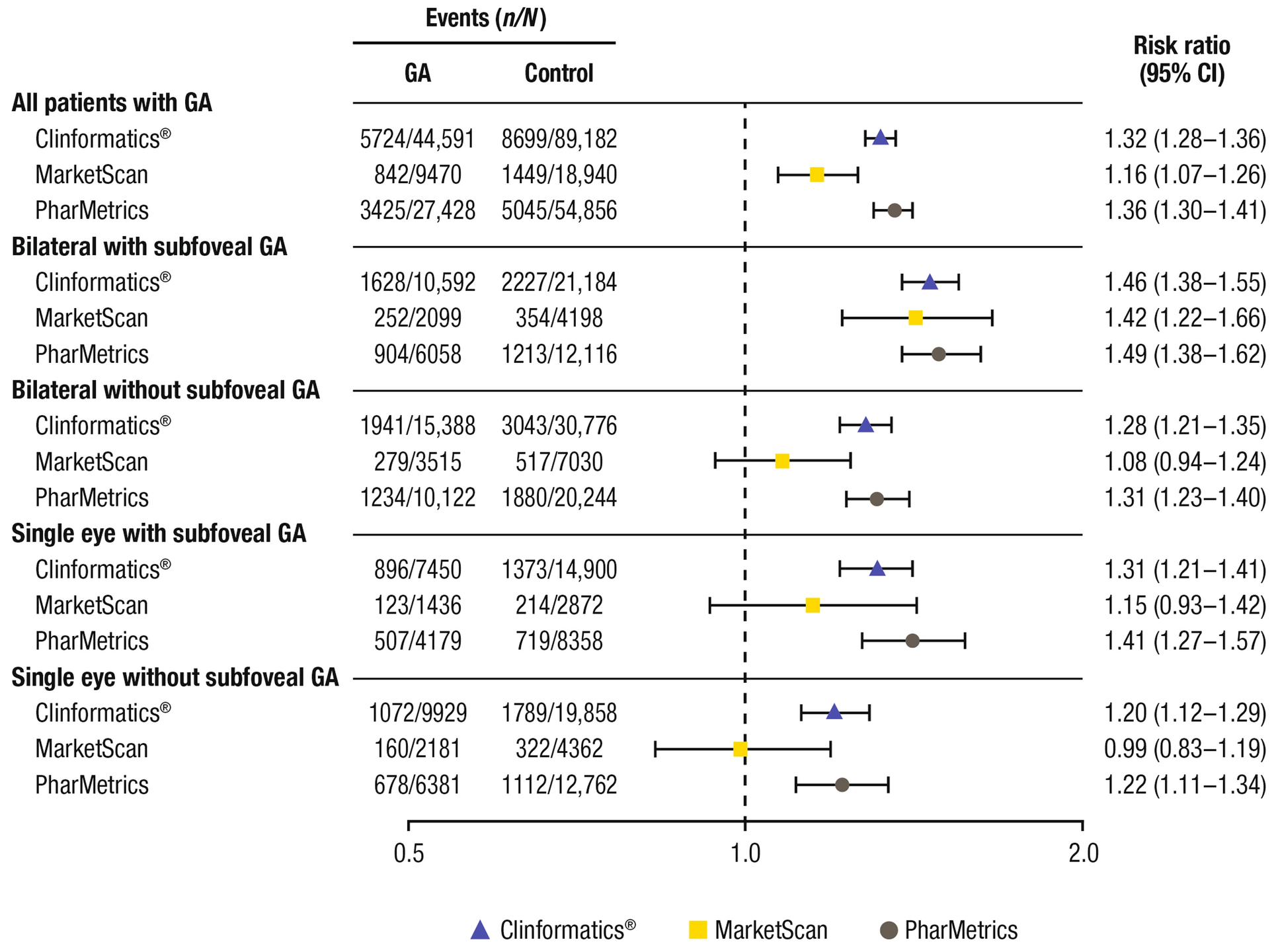
We identified patients aged ≥ 50 years with GA as defined by the International Classification of Diseases, Tenth Revision (ICD-10; H35.31x3 and H35.31x4; Table S1 in the Supplementary Material) on or after October 1, 2015. Date of first GA diagnosis after October 1, 2015 was considered the index date for the GA cohort. Patients were required to have at least 12 months of continuous enrollment in their health plan before the index date to be eligible for inclusion. Patients with a diagnosis of GA before the index date, with diagnostic codes indicating wet AMD at any time point (International Classification of Diseases, Ninth Revision [ICD-9]: 362.52, ICD-10: H35.32x) or indicating “single eye, with and without subfoveal involvement” on the index date, or with evidence of regression of GA, were excluded. Patients with GA were classified according to the eye(s) involved (single or bilateral) and location of the lesion (foveal or subfoveal). A group characterized as having bilateral GA with and without subfoveal involvement was also assessed to account for the potential misclassification of patients to the subgroups of patients with or without subfoveal involvement; these results are not reported here because of the small sample sizes.
A control cohort was formed on the basis of a 25% random starting population extracted from the overall sample population in the three datasets. Individuals were further restricted to those aged ≥ 50 years with no diagnosis of GA or AMD during the study period (based on the absence of ICD-9/10 diagnosis codes [ICD-9: 362.51, ICD-10: H35.31x]). A random index date was applied using a uniform distribution over the study period. Individuals in the control cohort were required to have at least 12 months of continuous enrollment in their health plan before the index date.
Patients with GA were followed from the index date until the first of the following events: the end of the first enrollment segment after the index date; the end of the study period; 4 years after the index date; the occurrence of an outcome of interest; or death due to any cause (Fig. S1a in the Supplementary Material). The start and end of data windows for the enrollment of control individuals were January 1, 2000 to December 31, 2022 for Clinformatics® and January 1, 2000 to June 30, 2022 for MarketScan and IQVIA (Fig. S1b in the Supplementary Material).
Propensity Score Matching
Individuals with and without GA were matched in a 1:2 ratio based on 5-year age bands at the index date, sex, and the index year, and then were further matched on the basis of selected patient and clinical characteristics (Table S2 in the Supplementary Material), using propensity score matching with logistic regression using a caliper distance of 0.2 [18]. The characteristics used in propensity score matching included demographic information, Charlson Comorbidity Index (CCI) conditions, ophthalmic conditions, the use of a nursing home or assisted living facility, antivascular endothelial growth factor therapy, and known risk factors for fracture. Propensity scores were calculated using a logistic regression model where the probability of having GA versus not having GA or AMD was conditional on the selected patient and clinical characteristics. The greedy nearest neighbor algorithm was used to select the closest match first, then the closest remaining match, and so on until no further acceptable matches were available.
Falls and Fractures
Incident falls and fractures that occurred following the diagnosis of GA after the index date were assessed individually. Falls were identified based on the presence of at least one principal/first or second ICD code for falls (Table S3 in the Supplementary Material). In patients who experienced multiple falls, a fall that occurred at least 30 days after the first event was classified as a new event, and a fall that occurred less than 30 days from the first event was classified as the same event.
Fractures were identified by the presence of at least one principal/first ICD code for fracture category by fracture location; or a secondary diagnosis, identified by accompanying current procedural terminology codes for site-specific fracture repair procedures (Table S3 in the Supplementary Material). Fractures occurring at a different body site at least 30 days after the first fracture were classified as new; fractures at different body sites that occurred less than 30 days from the first fracture were considered the same event. Fractures at the same site that occurred within 1 year of each other were also categorized as the same event.
Health Care Resource Utilization
Health care resource utilization (HCRU) data within 2 years after the index date were assessed, including the frequency of all-cause hospitalizations, ED visits, outpatient visits, and the use of a nursing home or assisted living facility.
Statistical Analyses
Descriptive statistics including frequency and proportion were used to describe categorical/binary variables, and mean, standard deviation, median, interquartile range (IQR), minimum, and maximum were used to describe continuous variables. Patients with GA and control individuals (all patients and those within patient subgroups [based on single/bilateral and subfoveal involvement]) were compared using a generalized linear model, and relative risks (RRs) and 95% confidence intervals (CIs) were calculated to describe the risk of fracture/fall. Sample selection and creation of analytic variables were performed using the Instant Health Data software (Panalgo, Boston, MA). Statistical analyses were undertaken with R, version 3.2.1 (R Foundation for Statistical Computing, Vienna, Austria) and SAS Enterprise Guide 7.1 for Windows (SAS Institute, Cary, NC).
Ethical Approval
This study was based on de-identified data collected from three US health care claims databases and did not include human participants; as such, this analysis was exempt from institutional review board oversight and informed consent was not required or obtained.





Comments (0)