Given the escalating and urgent threat posed by drug-resistant Gram-negative pathogens, there is still an unmet medical need for additional antibacterials against CR pathogens [22]. Major mechanisms of antimicrobial resistance are efflux pumps, porin channels, and β-lactamases. Cefiderocol’s siderophore-based mechanism of action is what is unique and addresses efflux and porin channels [23,24,25]. Besides, cefiderocol was the only agent stable against all classes of β-lactamases and was expected to be a promising treatment option [26]. So far, all the studies on the PK and PK/PD of cefiderocol have exclusively focused on other ethnic groups. Consequently, it is crucial to address the gaps in knowledge regarding the PK and PK/PD profiles of cefiderocol in the Chinese adult population.
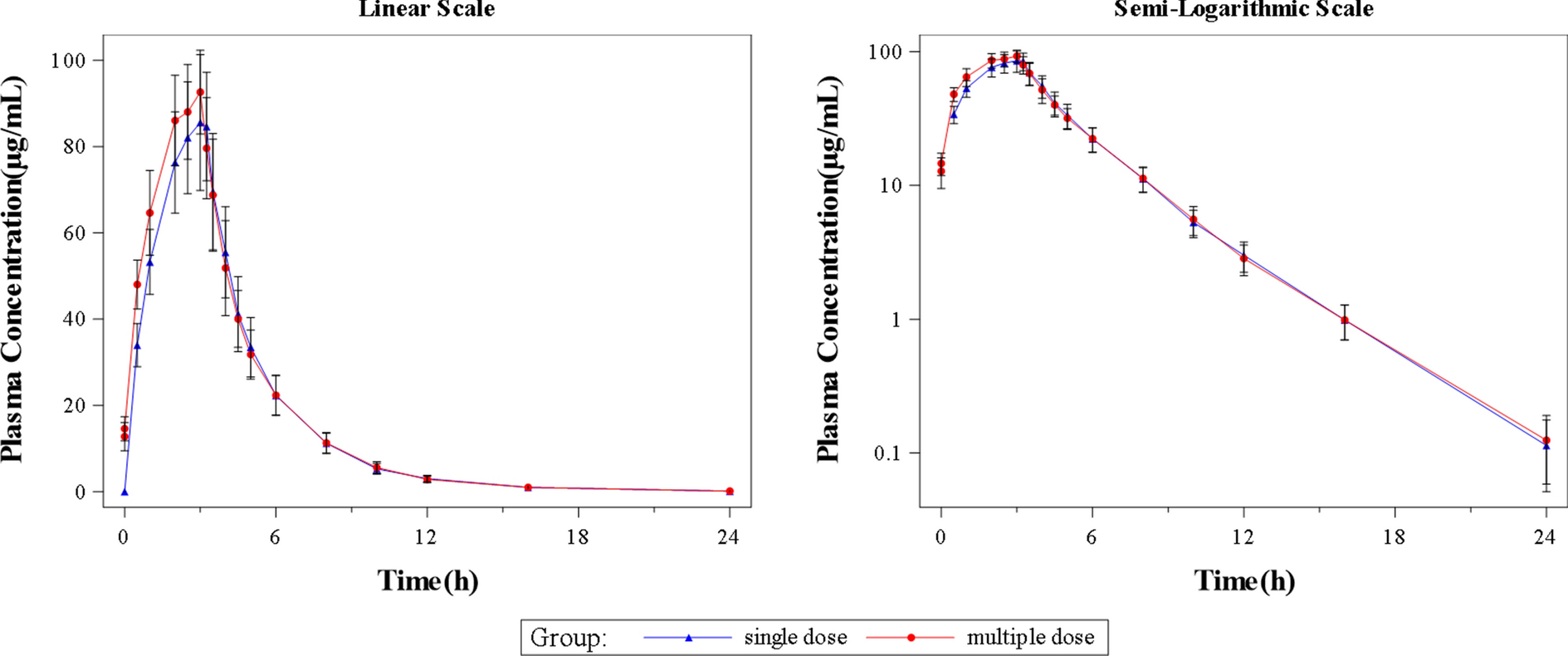
To the best of our knowledge, this is the first study demonstrating the favorable safety and PK properties of cefiderocol, the first siderophore cephalosporin in healthy Chinese subjects. Single- and multiple-dose administrations of 2 g cefiderocol were well tolerated, and drug-related TEAE were mild, with no serious adverse events or deaths reported; these findings are consistent with those from previous phase I studies [11, 13, 14]. No trial-related adverse events (AEs) of special interest, such as Clostridium difficile-related AEs, liver-related AEs, seizures, hypersensitivity reactions, and iron homeostasis-related AEs, were observed with cefiderocol [27].
In this study, individual PK parameters were further estimated with an empirical Bayesian method by NONMEM (version 7.4.4) based on the population PK model previously reported, which described the observed concentration data in Chinese individuals well [19]. The estimated PK parameters were compared among the Chinese, Japanese, and non-Asian healthy subjects. Our findings suggest that PK properties of cefiderocol in the Chinese healthy subjects were comparable to those of other healthy subjects from other ethnicities, and thus the existing findings and conclusions for cefiderocol might be applicable for Chinese people. According to the published population PK models that described cefiderocol PK well for each renal function group [11], we learned 2 g cefiderocol q8h with 3-h infusions provided adequate efficacy for patients with normal renal function, a reduced dose and/or extended dosing interval could be selected for patients with impaired renal function, and a supplemental dose immediately after hemodialysis was proposed. The PK profiles and dosage adjustment for patients with impaired renal function or undergoing hemodialysis serve as a reference, and the gap in cefiderocol studies among Chinese, Japanese, and non-Asian is expected to be bridged on the basis of these outcomes.
A dose fractionation study demonstrated the superiority of %fT>MIC in describing the in vivo efficacy of cefiderocol, compared with the other two PK/PD indexes [28]. Nakamura and colleagues obtained PD targets of cefiderocol in neutropenic murine models of thigh and lung infections caused by multiple GNB isolates [16]. For all Gram-negative pathogens, we selected a target of an average %fT>MIC of 75.0%, as well as the mean %fT>MIC needed to achieve a 1-log10 reduction in CFU for different strains, and estimated the PTA and CFR values with the dosage regimen of 2 g cefiderocol q8h via 3-h infusion, based on the two-compartment PK model we built. The results demonstrate that the recommended dosage regimen can achieve adequate efficacy against pathogens with a MIC up to 4 μg/mL (both PTA and CFR > 90%), supporting 3-h infusion of 2 g cefiderocol q8h as an effective therapy in the treatment of GNB infection, including those caused by Enterobacterales, P. aeruginosa and Acinetobacter spp. A previous study by Kawaguchi et al. established a PPK model using the blood concentrations of 91 non-infected patients and 425 patients with pneumonia, bloodstream infection, and cUTI, which suggested that the PTA for 75.0% fT>MIC was also exceeding 90% against MICs up to 4 μg/mL regardless of infection site or renal function group; 90% of PTA even covers pathogens with MICs as high as 8 μg/mL at the same PD target (75.0% fT > MIC), in all infection sites and renal function groups except for patients with normal renal function suffering from bloodstream infection and pneumonia [19]. However, our results suggested that the simulated PTA for Chinese healthy subjects was < 90% at MICs of 8 μg/mL. This inconsistency might result from the slightly slower PK elimination phase of patients and the accordingly higher Ctrough than healthy subjects, even if the patient does not have renal dysfunction. In the phase 3 studies, the geometric means of estimated Ctrough were 16.3 μg/mL (for the CREDIBLE-CR study [10]) and 12.7 μg/mL (for the APEKS-NP study [9]) in critically ill patients, which is higher than that of healthy subjects (11.2 μg/mL according to our results). Therefore, the higher PTA at MICs of 8 μg/mL is expected to be achieved for Chinese patients.
S. maltophilia is identified as an emerging MDR opportunistic pathogen that confers intrinsic resistance to multiple classes of antibacterials including β-lactams, creating a lack of viable treatment options [29]. This study demonstrates that cefiderocol exhibits outstanding efficacy against S. maltophilia with MICs reaching up to 8 μg/mL (both PTA and CFR > 90%), making it a promising antibacterial agent to address the existing gaps in effective treatment options for S. maltophilia.
The CLSI-approved MIC breakpoints for cefiderocol are ≤ 4 (susceptible), 8 (intermediate), and ≥ 16 mg/L (resistant) for Enterobacterales, P. aeruginosa, and A. baumannii. For S. maltophilia, the breakpoints are ≤ 1 mg/L (susceptible) and > 1 mg/L (nonsusceptible) [21]. In a study involving 1158 CRE isolates collected from multiple centers in China, 97.3% of the isolates exhibited susceptibility to cefiderocol; however, a significant percentage of Escherichia coli showed high-level resistance to cefiderocol [30]. The MIC50 and MIC90 of cefiderocol against all isolates were both 2 μg/mL. Similarly, the MIC90 of cefiderocol against Klebsiella pneumoniae isolates (n = 789) and Enterobacter cloacae isolates (n = 101) also measured 2 μg/mL. These results imply that the current dosage regimen can effectively address these CR pathogens, as per the PK/PD breakpoints (MIC 4 μg/mL) we acquired. Furthermore, for K. pneumoniae carbapenemase (KPC)-producing isolates (n = 569) and imipenemase (IMP)-producing isolates (n = 49) both with the MIC90 of 2 μg/mL, great efficacy against nearly all of them was also expected to be achieved with this regimen. And for New Delhi metallo β-lactamase (NDM)-producing isolates (n = 351) with MIC50 of 2 μg/mL and MIC90 of 4 μg/mL, most of them could be covered, exhibiting satisfactory microbiological efficacy.
It is worth noting that our results are solely derived from a limited sample of 12 healthy subjects, and all the conclusions we obtained are dependent on the data of a small-scale phase 1 clinical trial, which only preliminarily predicted the efficacy of this cefiderocol dosage regimen among Chinese people. Undoubtedly, additional data for model optimization may be necessary, and further study still requires a larger sample size.





Comments (0)