
Remember me






Every two years, the NHANES study employs a sophisticated approach to choose a sample that accurately represents the U.S. population [20]. The primary objective is to assess the well-being and dietary condition of people in the United States. Approval for the survey protocol has been granted by The National Center for Health Statistics Institutional Review Board in order to uphold ethical standards. Furthermore, prior to being included in the study, all participants gave written informed consent. NHANES gathers a broad spectrum of information, such as demographics, dietary habits, medical examination outcomes, laboratory results, and questionnaire responses [21]. The information used in this research is accessible on the NHANES site, and does not require any ethical evaluation.
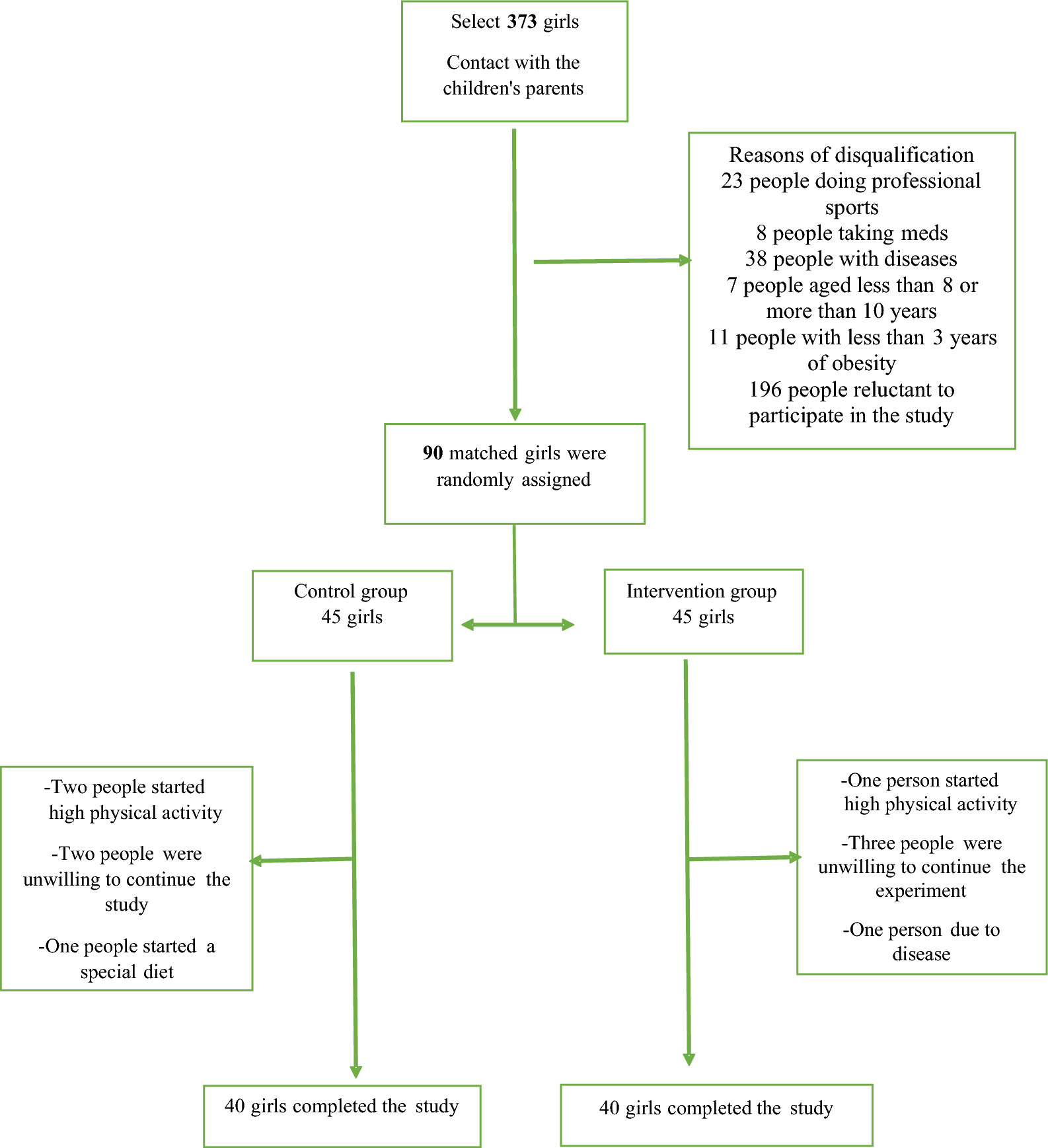
In the NHANES 1999–2000 cycle, 9,965 individuals participated in the study. Figure 1 displays the 2,859 participants who were 20 years old or above in the study sample. A total of 7,106 subjects were excluded from the study: 5,085 due to being under the age of 20, 735 due to incomplete H. pylori data, and 626 due to incomplete dietary vitamin B2 data. Additionally, 1,141 subjects were excluded due to missing data for covariates, including marital status (n = 438), poverty-income ratio (PIR; n = 537), smoking status (n = 8), educational level (n = 13), alcohol use (n = 137), hypertension (n = 42), diabetes (n = 50), and body mass index (BMI; n = 37). Ultimately, 2,859 participants were included in the final analysis. All protocols adhered to the principles outlined in the Declaration of Helsinki and followed the guidelines of the STROBE initiative for reporting observational studies in epidemiology.
Fig. 1 Dietary vitamin B2 intake
Dietary vitamin B2 intakeNutritional intake assessments were carried out during face-to-face interviews at the NHANES mobile examination centers. Participants underwent two 24-hour dietary recalls to gather dietary intake data. Interviewers who were trained conducted the first recall interview in person at the Mobile Examination Center (MEC). The follow-up interview occurred either over the phone or through mail within a timeframe of 3 to 10 days. Dietary evaluations were conducted by averaging the information from these two recalls (26). Dietary vitamin B2 intake on the first day was analyzed in accordance with NHANES analytic guidelines [22]. Vitamin B2 intake was analyzed by considering it in both continuous and categorical forms (Q1-Q4). Vitamin B2 intake quartiles (Q1-Q4) were established by dividing the distribution of vitamin B2 intake into four sections, representing varying levels of intake from low to high. The quartile ranges are as follows: Q1 (< 1.14), Q2 (1.14–1.64), Q3 (1.65–2.33), and Q4 (> 2.33).
H. pylori antibody measurementBlood samples were taken from individuals and frozen at -80 °C before being analyzed at the University of Washington following the NHANES guidelines. H. pylori IgG antibodies were tested with an ELISA kit from Wampole Laboratories in Cranbury, NJ to measure the level of antibodies [23]. Participants were categorized into two groups based on their H. pylori seropositivity using the standard ELISA cut-off value: seropositive (OD value ≥ 0.9) and seronegative (OD value < 0.9) [24, 25].
CovariatesThe study considered several potential confounding factors by referencing prior research and utilizing clinical judgment. Included in these considerations were age, sex, marital status, poverty to income ratio (PIR), level of education, body mass index (BMI), smoking status, alcohol intake, diabetes, high blood pressure, and C-reactive protein (CRP). Age was displayed as a continuous factor, whereas gender was evaluated as a categorical variable with options for male and female. Marital status was classified as either being married or living with a partner, or living alone. The PIR (a ratio of family income to poverty threshold) was utilized to assess socioeconomic status, categorizing individuals into low (PIR < 1.3) and high (PIR ≥ 1.3) groups according to their PIR value compared to 1.3. Educational level was classified into three groups: less than 9 years, 9 to 12 years, and more than 12 years. BMI was classified into three categories: normal weight (BMI less than 25 kg/m2), overweight (BMI between 25 and 30 kg/m2), and obesity (BMI greater than 30 kg/m2). Smoking status was classified as either non-smoking or smoking according to the response to the SMQ 020 (Smoked at least 100 cigarettes in life). Likewise, alcohol consumption was divided into non-alcohol consumption and alcohol consumption based on the answer to the questionnaire (ALQ100: Had at least 12 alcohol drinks/1 year? ). Diabetes diagnosis in the study was based on the Diabetes Questionnaire (DIQ) question DIQ010, which asked participants if they had ever been informed by a doctor or health professional that they have diabetes or sugar diabetes. Individuals who answered yes to the DIQ010 inquiry were categorized as having diabetes. In this research, hypertension was identified using question BPQ020 from the Blood Pressure & Cholesterol Questionnaire (BPQ), which asked participants if they had been diagnosed with hypertension by a healthcare professional. Participants responding affirmatively to the BPQ020 question were categorized as having hypertension. Laboratory measures included C-reactive protein (CRP).
Statistical analysisThe research separated the information into two groups: continuous and categorical variables. Continuous variables were further categorized based on the distribution’s normality. The Student’s t-test was utilized for comparing continuous variables that followed a normal distribution, and were presented as mean with standard deviation. Variables that did not follow a normal distribution were presented as median with interquartile range (IQR) and compared using the Wilcoxon rank-sum test. Categorical variables expressed as percentages were compared using the chi-squared test. To evaluate the significance of variations among groups divided by quartiles of vitamin B2, either the Kruskal-Wallis test or one-way analysis of variance was employed.
Multivariate logistic regression analysis was used to assess the intake of vitamin B2 in the diet, both as a continuous and categorical factor, with results shown as odds ratios (ORs) and 95% confidence intervals (CIs). Logistic regression analysis utilized three different models. Model 1 had no factors, while model 2 considered age, gender, and ethnicity, and model 3 accounted for all potential influences from model 2 as well as BMI, tobacco use, drinking habits, diabetes, high blood pressure, and C-reactive protein levels, total calories intake, total protein and total carbohydrate intake. Trend tests were conducted by incorporating the median of every quartile as a continuous variable in the models. The models were specified as follows: Model 1: unadjusted. Model 2 was modified to account for age, gender, and ethnicity. Model 3: adjusted for all confounders. Sensitivity analysis was conducted based on different cut-off value of dietary vitamin B2.
Data analysis was conducted with R software version 4.1.1, the R survey package version 4.1.1, and Free Statistics software version 1.9.2from R Foundation for Statistical Computing in Vienna, Austria [26]. Statistical significance was determined with a two-tailed p-value less than 0.05. This cross-sectional study was reported in accordance with the guidelines outlined in the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement [27].
Comments (0)