
Remember me
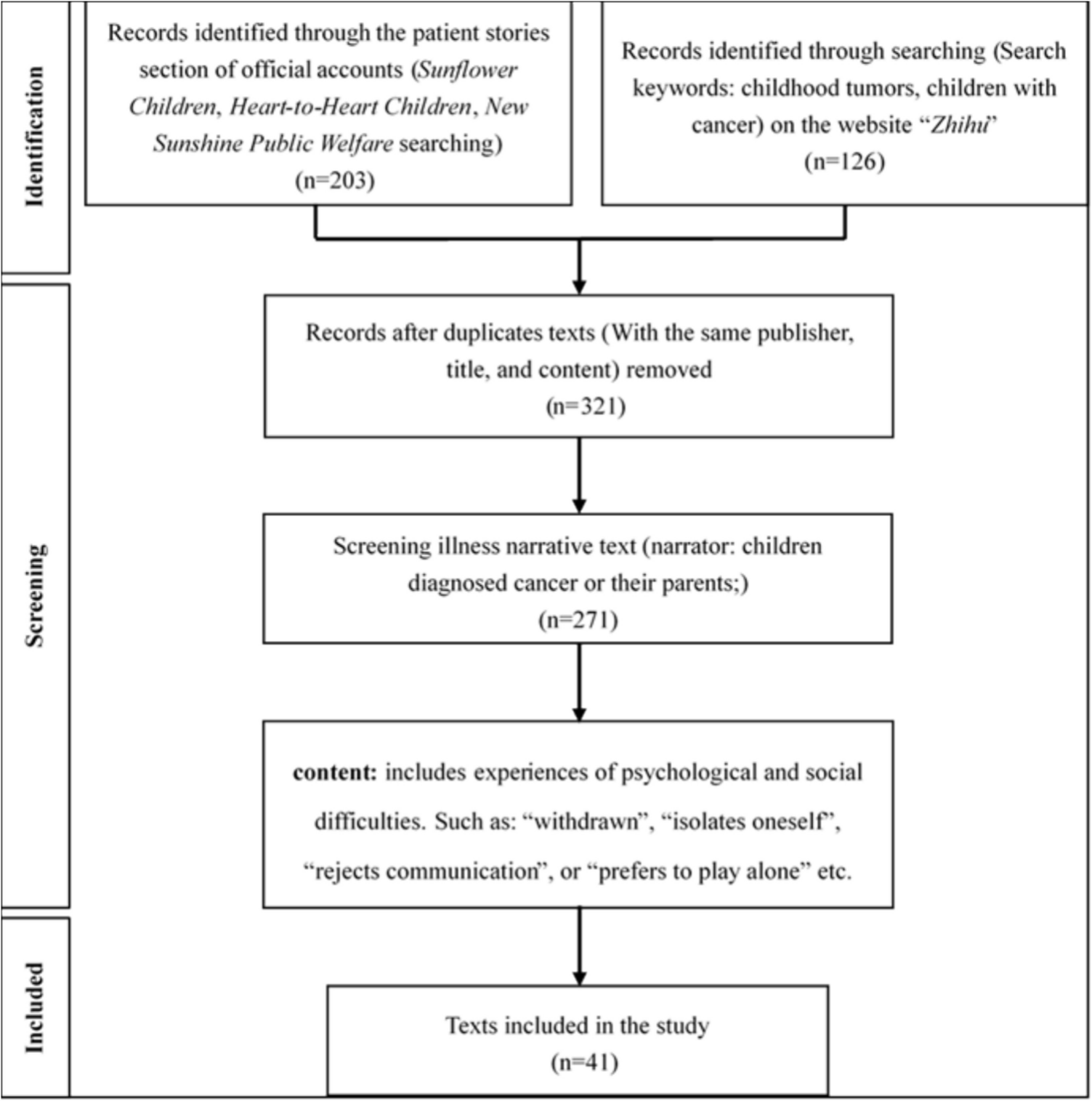

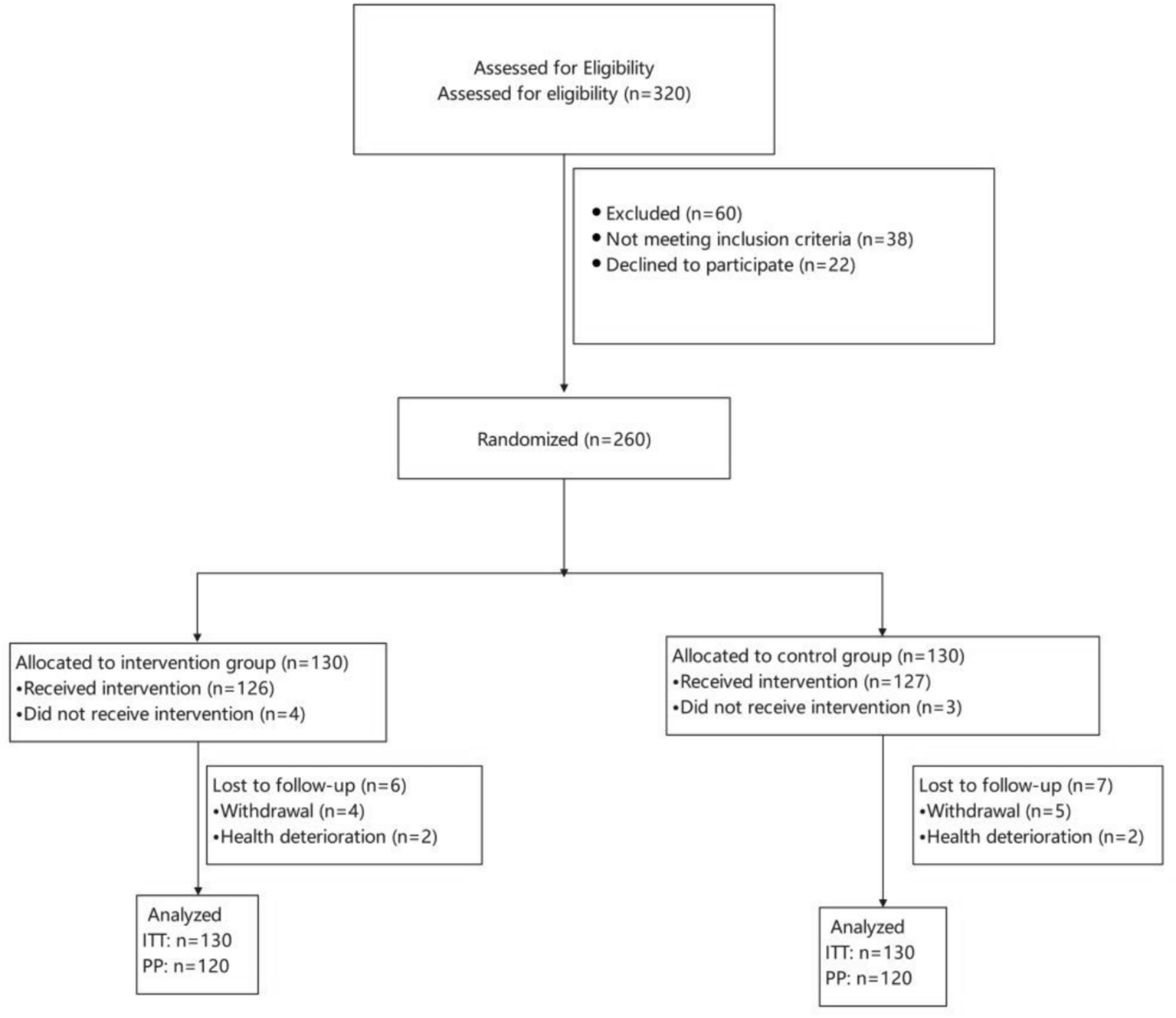
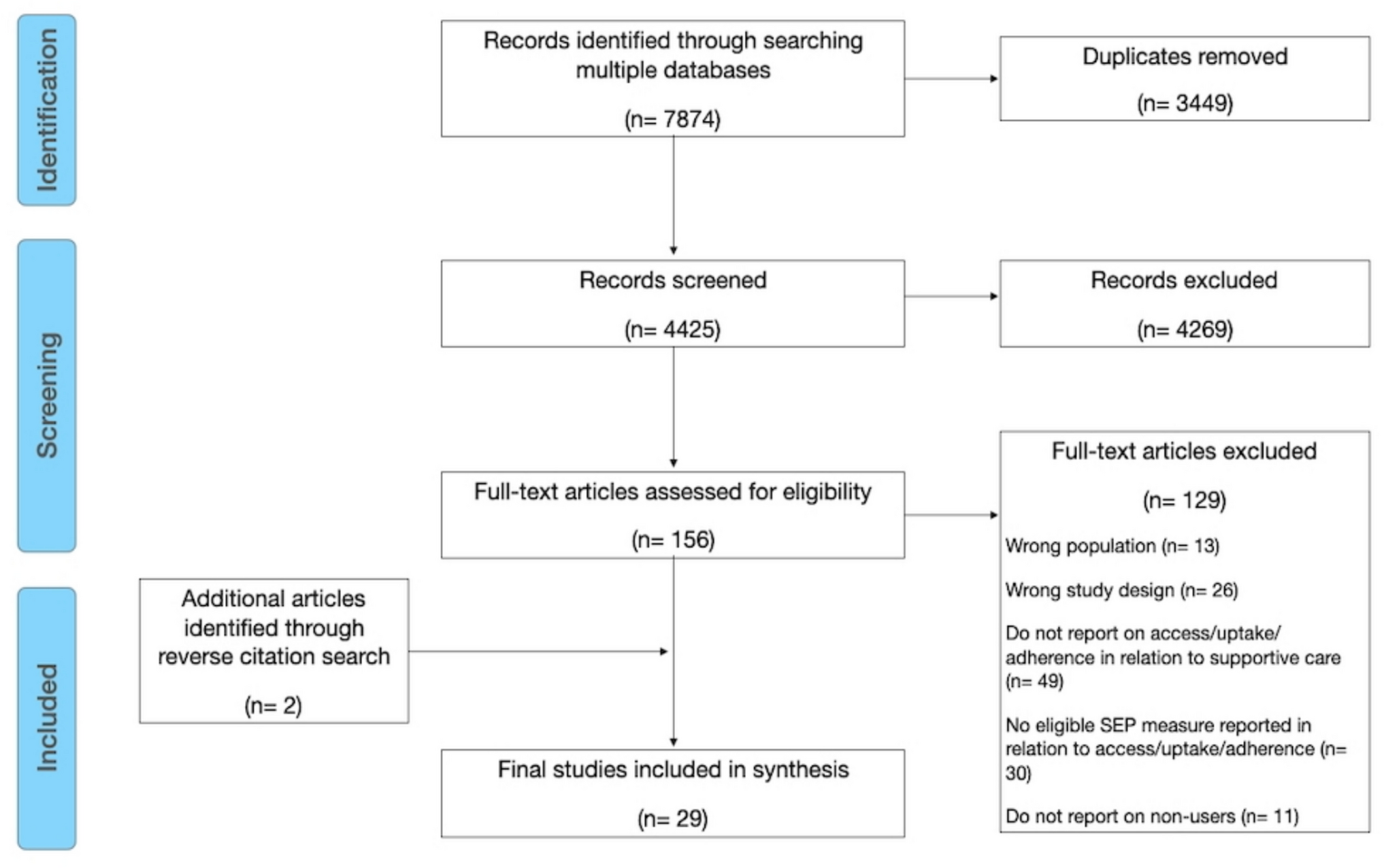
A total of 3226 articles were initially identified through database searches and hand searching (n = 4) (Fig. 1). Following removal of 1810 duplicate articles, 1420 remained for review. Title and abstract reviews were undertaken by two researchers (RB and NH), with 1392 articles not meeting the inclusion criteria. The remaining 28 studies underwent full text review. A further 15 studies did not meet the inclusion criteria, leaving 13 studies [34,35,36,37,38,39,40,41,42,43,44,45,46] that explored the lived experience of men on active surveillance for prostate cancer. A summary of included studies is in Table 1.
Fig. 1
Flowchart of studies through the review process
Table 1 Summary of included studiesStudy characteristicsStudy settings and designsSeven of the 13 studies were conducted in the USA [35,36,37, 41,42,43, 45], three studies were set in Canada [39, 40, 44], with one each from the UK [34], Australia [38], and the Netherlands [46]. All studies were conducted between 2005 and 2021. In eight of the studies participants were recruited through clinics, patient databases, or medical records from large tertiary treatment centres [34, 37, 39, 40, 42, 44,45,46]. Two studies recruited participants through participating urologists’ patient records [36, 43]. One study used the urologists practice database of suitable patients in addition to a local cancer registry [35]. In one study, it was not clear where the patients were recruited, although it identified that interviews were conducted with patients through two academic institutions [41]. In the remaining study, recruitment was through a private urology practice, an integrative cancer centre or a public hospital active surveillance clinic [38].
All studies were qualitative in design with the exception of one that employed a mixed methods approach [42].
ParticipantsRecruitment of participants was purposive in all studies. The numbers of participants ranged from 7 to 37. Age of participants ranged from 47 to 88, with mean age ranging from 61 to 70. Four of the studies did not report age range or mean age [37, 38, 41, 42].
Data collection methodsSemi-structured interviews were used for data collection in ten studies [34, 38,39,40,41,42,43,44,45,46]. The remaining three studies utilised focus groups for their data collection [35,36,37].
Risk of bias in studiesThe quality of all included studies per the CASP tool [32] was high (refer Supplementary Table 2). The aim of the research was clearly identified in all studies and appropriate methodology was utilised to undertake qualitative research. Ethical considerations were evident in all studies and recruitment and data collection approaches were well articulated. Findings from each study were clear and the value of the research was evident. The ability to understand the relationship between the researcher and participants was only evident in three of the studies [34, 36, 38].
ThemesTwo overarching analytical themes were identified in this meta-synthesis: (i) men on active surveillance live with a lack of certainty; and (ii) re-establishing agency (i.e. a feeling of control over actions and their consequences [47]) drives resilience and facilitates confidence in active surveillance (Supplementary Table 3). Lack of certainty on active surveillance is derived from men feeling a loss of control over their health and/or lives as they continue to live with an essentially untreated cancer. This lack of certainty induces a cyclical stress response of ongoing worry and anxiety and a resultant loss of agency, which further drives the stress cycle. However, re-establishing agency alleviates the stress response, promotes resilience, and facilitates confidence in active surveillance as a treatment choice (Fig. 2).
Fig. 2
Conceptual diagram of the lived experience of active surveillance for men with prostate cancer
i. Men on active surveillance live with a lack of certainty My cancer is not being treated; it’s still growing inside me. It worries meMen live with a lack of certainty whilst on active surveillance driven by ongoing awareness of an ‘untreated’ cancer remaining in their body [46] describing that this worry never ‘leaves their mind’ [36, 46]. Clinicians’ explanations of low-grade, low-aggressive, or slow-moving disease do not ameliorate these concerns [40, 44], and any time cancer is mentioned men report feeling frightened [43].
The tests aren’t reliable, what if it gets away?Additionally, men are worried that their cancer will progress undetected, and their opportunity for cure will be missed [35]. The fear of undetected disease progression is perpetuated by men linking any new physical symptoms directly to their cancer and seeing symptoms as signs of advancing disease [43], aided by a lack of clear information as to what indicates if progression is occurring [37]. The monitoring tests associated with active surveillance do not drive optimism in treatment. Men are dubious as to their efficacy and reluctant to be reassured by results as they lack trust in the tests to adequately detect disease progression [38, 42, 46]. The routine follow-up required as part of active surveillance exacerbates these worries with men detailing the anxiety they suffer at the time of follow-up [34, 39] and waiting for the results [34]. Collectively, these factors lead men to question their choice of an observational strategy versus curative treatment [43].
I don’t have any trust in my treating teamAdding to their lack of certainty, the trust men develop in their treating team influences their experience of active surveillance. Men describe a feeling of disconnect, no rapport or connection [44], and a lack of responsiveness to questions [44] as being detrimental to developing trust in their treating team, and establishing confidence in active surveillance to safely monitor their disease. Men have also detailed that conflicting information and advice from health care team members impedes trust in the team [38].
There is so much information out there, how do I know what I can trust?Men actively seek information on their disease and their treatment, beginning early following diagnosis [46]. Men report being presented with an abundance of information on prostate cancer [36]; however, information is not always easy to understand [37] and that the information available can often be contradictory and confusing [35]. Men are concerned about the ability to verify the integrity of information available and seek sources that can be trusted and reliable [37], provide clear information relevant and specific to active surveillance, and detail new developments related to active surveillance [36].
Discordant terminologyDo I have cancer or not?
Discordant terminology used by treating teams at diagnosis and when describing active surveillance contributes to men’s lack of certainty. Men describe members of the treating team avoiding the term ‘cancer’ altogether at diagnosis, instead describing a presence of ‘…some atypical cells’ [44] or indications of cancer [40] and telling men ‘…you don’t have a problem’ [38].
Cancer should be treated.
Upon commencing active surveillance, men explain that treating teams have described active surveillance as ‘…not doing anything’ [44] or ‘…leaving it as it is’ [44] rather than a structured treatment regime designed to monitor disease progression, with the end goal to offer further curative treatments [48]. This can result in men not believing that they are on a recognised treatment strategy [40]. Men also detail pressure from family and friends to properly ‘treat their disease’ adds to their stress as they feel required to defend their decision to commence and continue active surveillance [36].
What am I waiting for?
Furthermore, men describe terminology being used by treating teams that is discordant with the clinical description of active surveillance, terms such as ‘watch and wait’, ‘wait and see’, and ‘watchful waiting’ [35,36,37, 44], which can result in men not comprehensively understanding their treatment and further adding to confusion and lack of certainty.
ii. Re-establishing agency drives resilience and facilitates confidence in active surveillanceMen seek to maintain agency in their treatment, i.e. having the capacity to initiate and manage actions in response to awareness and ownership of health-related needs [8], enabling them to feel some control. This in turn promotes resilience, the successful adaptation to challenging life experiences through behavioural flexibility [49], to cope with the lack of certainty they experience with active surveillance and promotes confidence.
They are going to watch me closely, on a structured programThe knowledge that they are on a surveillance program with structured specifics of when and what follow-ups are required [34, 39, 41, 45], and that the treating team have the skills to identify and treat progressing disease [45], promotes confidence for men and supports their ability to develop resilience to the lack of certainty they face, and adhere to their chosen treatment [40].
Trust in the treating team and test results promotes confidenceIn contrast to the impact of sub-optimal therapeutic relationships, feelings of trust in their treating team enhances men’s resilience, supporting them to feel more confident in active surveillance [35]. Factors that promote trust in the treating team for men include professional qualifications and clinical experience [38, 44], feeling that their team are good at what they are doing and [41] know them and their medical history [35], reviews, and recommendations from peers and/or websites [37], and positive experiences from team members manner and style [44] all leading to men having trust in their team [35, 36, 41]. Consistency in advice and recommendations from clinicians and treating teams is also reassuring for men, adding to their confidence in active surveillance [35, 41]. Feeling they have received information that meets their needs also promotes agency for men, supporting their resilience and confirming they have chosen the correct treatment. Men describe that information provision to the level of their need and understanding is reassuring, and that their treating team is a great source of information to them [37, 46]. Men’s confidence in their active surveillance is further buoyed by favourable clinical results as they provide men with objective measures that their treatment is successfully monitoring their disease [35,
Comments (0)