Study design and participants
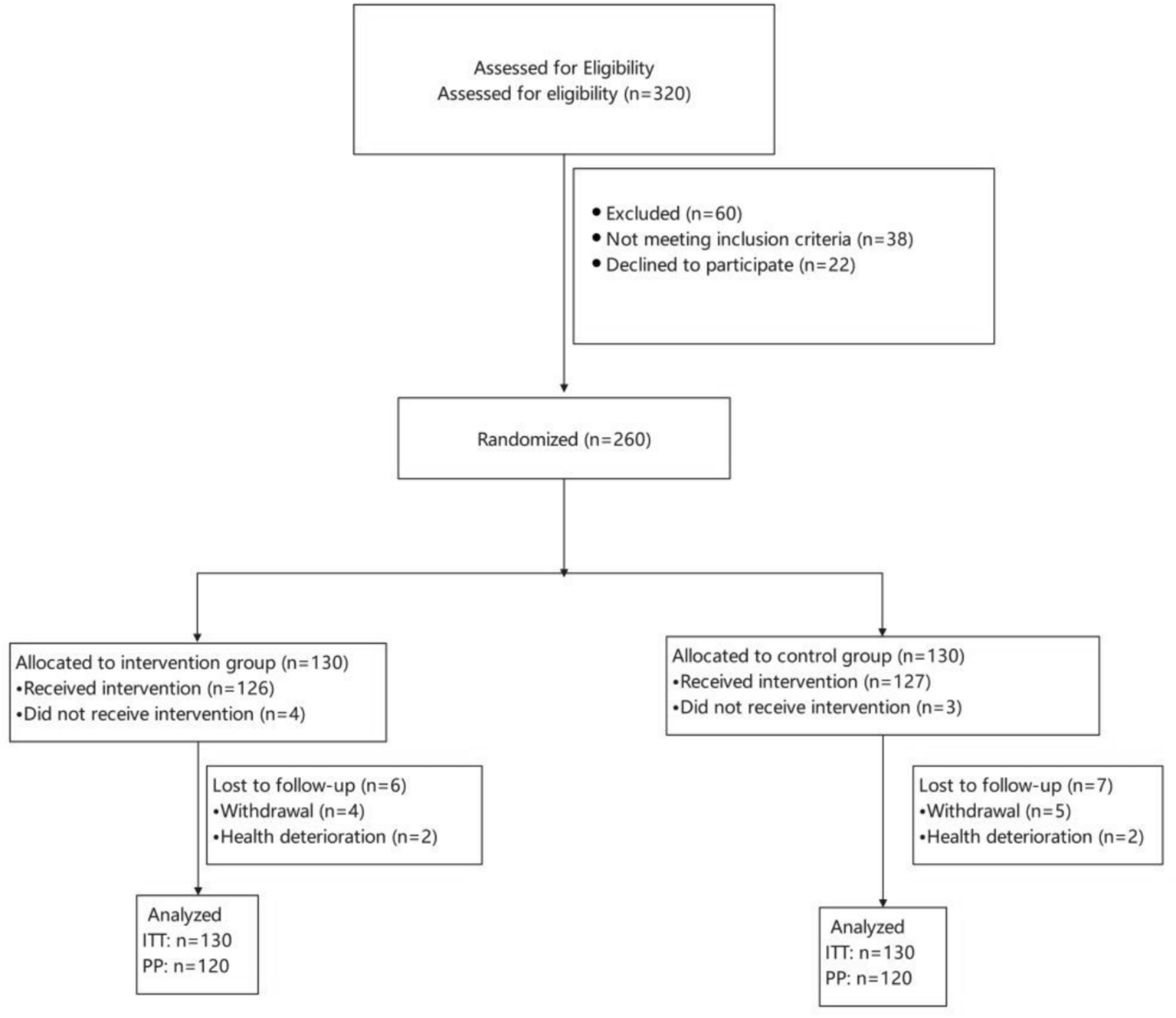
This study prospectively recruited 48 volunteers to enroll between September 2022 and December 2023, 24 each in the cancer chemotherapy (C +) and healthy control (HC) groups. Each participant was enrolled after eligibility checks with written consent after providing informed consent for the study. Measurements were completed before chemotherapy or baseline assessments and then after 6-month follow-up assessments and were evaluated under the same environmental conditions. Based on previous neuroimaging studies [20, 21], we estimated the feasible number of participants from previous outpatients at our single institution and determined a sample size of 20 for the C + group. To account for a potential 20% dropout rate, we increased the sample size estimate to 24 for the C + group. Similarly, with 24 cases in the age- and sex-matched HC group, a total of 48 cases were included in the study. This study was approved by the Ethical Review Committee for Epidemiological Research of Hiroshima University (E2022-0061).
The C + group included outpatients at the Hiroshima University Hospital who were to begin their first course of chemotherapy following a diagnosis of gastrointestinal cancer (colorectal, gastric, or esophageal cancer). The inclusion criteria for the C + group were as follows: (1) individuals who were at least 20 years and < 85 years old, (2) individuals who met the diagnostic criteria for gastrointestinal cancer, (3) individuals who were scheduled to start the first course of chemotherapy treatment, (4) individuals with no anemic symptoms and a hemoglobin level of > 8.0 g/dL on a blood test, (5) individuals with an Eastern Cooperative Oncology Group-performance status score (ECOG-PS) of 0 or 1, (6) individuals whose first language is Japanese, (7) individuals scheduled for outpatient visits for at least 6 months, and (8) individuals who provided written consent to participate in this study. The exclusion criteria were as follows: (1) individuals with a history of chemotherapy treatment for cancer, (2) individuals with a diagnosis of dementia or cognitive decline equivalent to dementia (Mini-Mental State Examination, Japanese version (MMSE-J) [22, 23], less than 24 points), (3) individuals with a diagnosis of severe depression or psychiatric disorder, (4) individuals regularly using sleeping pills due to sleep disorders, (5) individuals with primary brain tumors, metastases, or disorders to the central nervous system, (6) individuals with a history of alcohol or drug addiction, (7) individuals with a history of opioid analgesic use due to cancer pain, (8) individuals with cachexia or other poor systemic conditions, (9) individuals with serious liver disease, renal disease, seizure disorder, cardiac complications, (10) pregnant and lactating women, and (11) other individuals judged to be inappropriate by the principal investigator. The HC group recruited healthy volunteers from staff or family members of patients in outpatient rehabilitation facilities and community centers in the same residential area. The inclusion criteria for the HC group were as follows: (1) individuals who were at least 20 years and < 85 years old, (2) independent in activities of daily living (Barthel Index > 85 points), (3) individuals whose first language is Japanese, (4) individuals live in a permanent residence and can be examined after 6 months, and (5) individuals who provided written consent to participate in this study. The exclusion criteria for the HC group were as follows: (1) individuals with a history of cancer diagnosis and chemotherapy treatment for cancer, (2) individuals with a diagnosis of dementia or cognitive decline equivalent to dementia (MMSE-J, less than 24 points), (3) individuals with a diagnosis of severe depression or psychiatric disorder, (4) individuals regularly using sleeping pills due to sleep disorders, (5) individuals with a history of cerebrovascular disease (stroke, neurodegenerative disease), (6) individuals with a history of alcohol or drug addiction, (7) individuals with a history of opioid analgesic use due to pain, (8) individuals with serious liver disease, renal disease, seizure disorder, cardiac complications, (9) pregnant and lactating women, and (10) other individuals judged to be inappropriate by the principal investigator. The systemic condition and medical history of the C + group were collected using information from electronic medical records or self-reported by the individuals; information for the HC group was collected by self-report from the individuals. It was planned to exclude from the analysis cases where follow-up data could not be obtained due to an individual’s unanticipated life events or individual intent. Individuals for whom follow-up data were not available due to unforeseen life events were planned to be excluded from the analysis.
Assessments and fNIRS measurements
During the eligibility check, the following information was collected from the individuals as sociodemographic factors related to cognitive function: age, sex, education level, marital status, and employment status. Clinical characteristics, including tumor stage, cancer site, line of therapy, and chemotherapy regimens, were collected from the electronic medical records at our facility. In both groups, the MMSE-J and the Japanese version of the National Adult Reading Test [24, 25] were used to assess cognitive functional screening and predict IQ as a cognitive reserve at baseline. In the C + group, the co-occurring symptoms of cancer-related fatigue, sleep disturbances, and pain were investigated through self-reporting; anemia was screened based on blood hemoglobin levels.
The Japanese version of FACT-Cog version 3 [15, 26] was used to assess subjective cognitive complaints. The FACT-Cog is a 37-item, 5-point questionnaire that assesses perceived cognitive decline and recommends the use of sub-items rather than the total score, as it is divided into four sub-items. The study used scores for perceived cognitive impairments (CogPCI: score range, 0–72) and perceived cognitive abilities (CogPCA: score range, 0–28).
The Japanese versions of the TMT (TMT-J) [12, 27], Rey auditory verbal learning test (AVLT) [28, 29], and verbal fluency test (VFT) [14, 30] were used to evaluate objective cognitive function. The performance time of the TMT-J was assessed for part A (a task to connect numbers in sequence) to measure the processing speed domain and part B (a task to connect numbers and letters alternately) to measure the executive function domain. The AVLT was used to assess the verbal memory domain, and the following main outcome measures were assessed: total number of words from the first to fifth (AVLT-sum) and number of delayed recalls (AVLT-DR/AVLT-7). A letter fluency task was selected for the VFT to assess the language and executive function domains. The total number of 3 mora generated per 60 s was recorded according to COWA, and the number of generated words and duplicate errors for each mora (/a/ /ka/ /shi/) were recorded.
Continuous-wave P-NIRS (HOT-2000, NeU Corporation, Tokyo, Japan) is a wireless device with a Bluetooth connection. The sampling rate was 10 Hz, and the wavelength of the near-infrared light was 810 nm. This device allows the measurement of changes in total hemoglobin (THb) concentration according to the modified Beer–Lambert law; the reliability of prefrontal cortex measurements compared to multichannel fNIRS has been demonstrated by prior P-NIRS devices [31]. The NVC response is the principle of fNIRS measurements, and THb is one of the representative indicators of fNIRS, which represents the sum of oxyhemoglobin (O2Hb) and deoxyhemoglobin (HHb) concentrations. In a typical NVC reaction, THb and O2Hb concentrations increase if HHb remains unchanged. The P-NIRS instrument incorporates a multi-distance optodesis method [32] that removes the skin blood flow component by implementing a short channel to compensate for the shortcomings of previous fNIRS studies [33]. Based on the International 10–20 method, the positions of the left and right channels were defined as the positions corresponding to the frontal pole (FP) on the Fp1 and Fp2 lines or the lateral region (corresponding to part of the ventral and dorsal prefrontal cortex) as the lateral prefrontal cortex (LPFC). The participants in the P-NIRS experiment were seated in a quiet environment. The experiment used a block design method, and the most commonly used phonemic fluency task was the cognitive task for the fNIRS experiment. Changes in cortical activity during a phonemic fluency task are known to be highly relevant to the prefrontal cortex measured as regions of interest [34]. Based on previous studies [35], a modified protocol was used, in which, after an initial 30-s rest period, a 120-s cycle consisting of a 30-s control task, a 60-s phonemic fluency task, and a 30-s recovery task was repeated three times. The control task consisted of repeated vocalizations of the Japanese vowels (/a/, /i/, /u/, /e/, and /o/). The VFT comprised two sets of three 60-s repetitions of one more as a phonemic fluency task (/shi/, /i/, /re/, or /a/, /fu/, /ni/).
Analysis
Representative values for sociodemographic data, clinical characteristics, and cognitive functional assessment are expressed as means or medians, depending on the skewness of the distribution of the descriptive data. The Shapiro–Wilk test was used to test for normality. To compare the baseline characteristics and clinical data between the groups, we used the two-sample t-test or Wilcoxon rank-sum test for continuous variables and the chi-square test for categorical variables. Several parameters of the objective cognitive assessment using NPTs were transformed into age-matched normalized scores (Z-score) based on previous studies to obtain consistent descriptive data [27, 29, 30]. The TMT-A, TMT-B, and VFT errors were flipped values of the Z-score used so that the positive direction of cognitive performance had a better score. Welch’s two-sample t-test was used to compare differences in changes between the groups in each cognitive function assessment. Missing data without follow-up assessments were excluded. To compare within-group data, the paired t-test or Wilcoxon signed-rank test was used. To calculate the percentage of CRCI incidence, PRO and NPT were based on the following methods: for NPT, the ICCTF-recommended criteria for CRCI were used, defined as ≥ ±1.5 SD of the standard for two NPTs or ≥ ±2.0 SD for one NPT [6]; for PRO by FACT-Cog, the clinically important difference in FACT-Cog was defined as subscale scores ranging from 6.4 to 10.3%, so we defined this as a decrease of at least 4.6 points (6.4% decrease) on the CogPCI score or at least 1.8 points (6.4% decrease) on the CogPCA [36].
For the fNIRS analysis, pre-processing of the raw data was performed using the statistical analysis software TOMATO (HOT-ANALYSIS; NeU Corporation, Tokyo, Japan). A median filter and moving average were used for noise reduction. First, the median filter was set to a time window of 1 s to reduce the spike noise caused by body movement. Subsequently, the moving average was set to 3 s to smoothen the waveform data. The smoothed waveform data were averaged, and a baseline correction was performed with the task start time set to zero. To allow for inter-channel and inter-subject comparisons, we converted the Z-score to represent the change in THb concentration. It was converted to a normalized averaging waveform by dividing by the standard deviation of the 20 s value of the control task. Matlab R 2023a (Mathworks, Inc., Natick, MA, USA) was used to analyze the fNIRS data after pre-processing. Linear mixed models to account for repeated measures were used for between-group and within-group comparisons of the fNIRS data. The model included random effects for each individual participant, while fixed effects included group (C+ and HC), period (baseline and follow-up), and task condition (control task and VFT task). Variance components were estimated using restricted maximum likelihood methods. The two-sided significance level was set at 5%. All statistical analyses were performed using JMP pro 17.0.0 (SAS Institute Inc., Cary, NC, USA).


Comments (0)