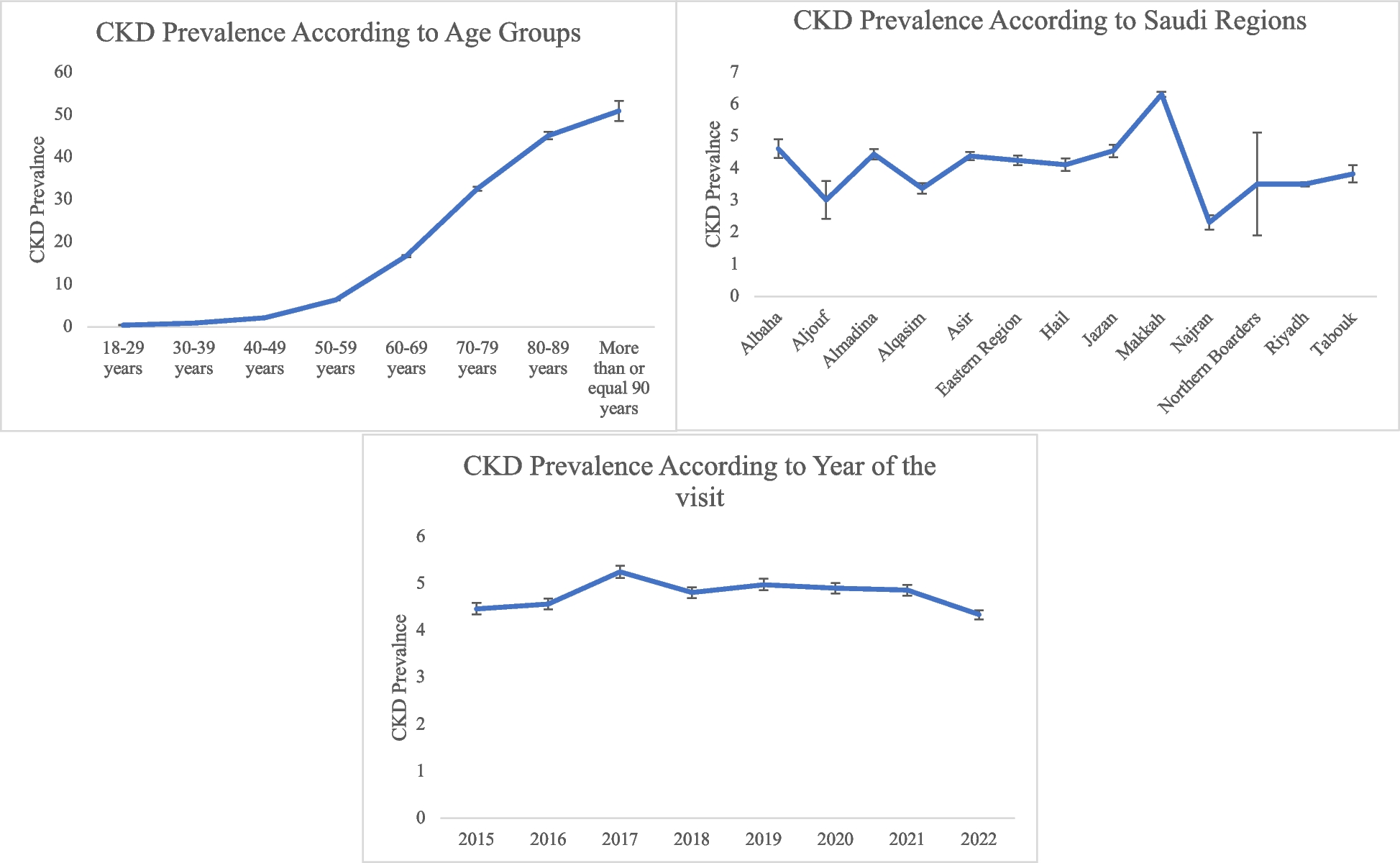
Over the 7-year study period, 691,388 people were tested at Alborg Laboratories, with 55.4% being male and 44.6% female. The most tested age group was 30–39 years, representing 27.3% of the cohort. We found that 4.76% (95% CI: 4.72–4.80) of people in Saudi Arabia have CKD, with most of them in stage 3 (3.50%). Men had a higher prevalence (5.83%, 95% CI: 5.76–5.90) compared to women (3.88%, 95% CI: 3.83–3.93), and the probability of CKD increased with age. For example, individuals aged 60–69 years had a CKD prevalence of 16.71%, while those aged 80–89 years had a much higher prevalence of 45.14%. Among the administrative regions, populations in Makkah (6.32%, 95% CI: 6.24–6.40) and Jazan (4.55%, 95% CI: 4.35–4.75) showed higher odds of CKD. Additionally, there was a significant association between CKD and HbA1c levels.
In this study, the prevalence of CKD was 4.76%, similar to the prior report of Alsuwaida et al., who identified a prevalence of 5.7% as determined by the MDRD-3 equation, and 5.3% when using the CKD-EPI equation [7]. A higher prevalence (13.8%) was reported by Mousa et al. [18]; however, that study was conducted on subjects with a significant family history of ESRD, which inherently places them at higher risk of CKD compared to the general population. Notably, the prevalence of CKD in Saudi Arabia appears to be lower than that in neighbouring countries. For instance, in Egypt, a prevalence of 13.0% has been reported [19], while a meta-analysis conducted in African countries revealed a pooled prevalence of 10.1%. Similarly, a study conducted in North Africa revealed a prevalence of 15.8% [20]. The variation in CKD prevalence across studies may be attributed to differences in sample size, characteristics of the study population, diagnostic criteria, and CKD assessment methodology. Understanding these disparities is crucial for accurately interpreting and contextualizing CKD prevalence estimates from diverse research settings.
The pathophysiology of CKD seems to exhibit sex-specific differences. It is believed that women progress at a slower rate than men [21, 22]. Hormones are presumed to play a role in shaping these sex differences, with potentially beneficial effects of estrogen or detrimental effects of testosterone [23]. In our study, the prevalence of CKD was higher among males than females. This aligns with previous reports of a higher prevalence of CKD among male patients from the study region [24] but contrasts with global reports of a higher prevalence among females [25].
It has been recognized that eGFR diminishes concomitantly with age [26]. This study found a statistically significant association between increasing age and the odds of having CKD in both univariate and multivariate analyses. The odds increased from 0.45% among adults aged 18–30 years to 50.94% among those aged 80–89 years. Similarly, in a Chinese study, the prevalence of CKD escalated from 7.4% among those aged 18–39 years to 18.0% among individuals aged 60–69 years and further to 24.2% among those aged 70 years and above [27]. Similar trends of rising CKD prevalence with age are evident in populations across the United States [28], Canada [29], and Europe [30].
Diabetes mellitus stands as one of the primary causes of CKD and ESRD. Kidney diseases in patients with diabetes can arise from various sources, including microvascular complications directly related to diabetes, a separate kidney disease of another origin, or a combination of both factors [31]. As expected, we found a statistically significant association between blood sugar levels (HBA1C) and CKD in the study population. The univariate model revealed a significant association between HbA1c levels and the odds of having CKD, with an OR of 1.43 (95% CI: 1.43–1.44). This suggests that for each unit increase in HbA1c (%), the odds of CKD increase by 43%, assuming other factors remain constant. Upon adjusting for potential confounders, the strength of this association was attenuated but remained statistically significant. The adjusted odds ratio was 1.10 (95% CI: 1.09–1.11), indicating that with each unit increase in HbA1c (%), the odds of CKD increase by 10% when other covariates in the model are held constant.
The association between CKD and hypertension is bidirectional in terms of pathophysiology. The prevalence of hypertension is estimated to increase significantly in the later stages of CKD [32]. Intensive blood pressure control can protect further kidney damage in CKD patients [33]. In our study, we found a significant association between CKD prevalence and systolic blood pressure. These findings align with previously published literature [34, 35]. Salt and water retention, activation of the renin angiotensin system, renal artery stenosis, endothelial damage, and drug-induced hypertension are the common mechanisms of hypertension development in CKD patients [36].
Despite that our CKD prevalence is similar to the study of Alsuwaida et al [7], The risk factors associated with CKD in our study differed from those reported by Alsuwaida et al. Several factors may explain this observation. First, our study had a substantially larger sample size (664,684 participants) compared to Alsuwaida et al.'s study (491 participants). Additionally, our participants were recruited from all 13 administrative regions of Saudi Arabia, whereas Alsuwaida et al.'s study included participants exclusively from Riyadh city.
Our study revealed significant variation in CKD prevalence across Saudi Arabia, ranging between 2.32% and 6.32%, with the highest prevalence observed in the Makkah and Jazan regions and the lowest in Najran and Alqasim. Previous national studies are not available to detect changes in prevalence over time, and overall data regarding CKD reporting in the country are lacking. The high prevalence of CKD in the Makkah region may be explained by the millions of older visitors who come annually for pilgrimages; hence, the findings may not represent the actual prevalence of CKD in the region. Jazan, meanwhile, is a coastal region in the south-eastern part of Saudi Arabia. A common factor between the Makkah and Jazan regions is that large portions of both regions are on the coast of the Red Sea. This geographical positioning, along with other environmental factors, could be linked to an increased risk of CKD. Environmental and lifestyle factors should be further investigated to understand the potential causes of higher CKD prevalence in these regions.
While a previous study reported a higher CKD prevalence among relatives of patients on Haemodialysis (HD) in the southern region [18], we did not find a meaningful increase in prevalence in the southern region compared to other parts of the country. This could be due to the nature of the sample in the previous study, which comprised people at higher risk of CKD, and the smaller sample size relative to our study.
Finally, the present study found only minimal association of CKD with hypertension, BMI, and lipid profile parameters. Given the nature of laboratory evaluations, the accurate diagnosis of diseases like hypertension can be challenging; therefore, caution should be taken when assessing these results.
Strengths and limitations
This study on the prevalence of CKD in Saudi Arabia is not just a data collection but a significant contribution to healthcare delivery and maintenance. It unveils the geospatial pattern of CKD over time, a crucial piece of information for policymakers and the Saudi health system. Moreover, the study delves into various sociodemographic factors associated with CKD; targeted screening programs should be implemented for high-risk populations, particularly males and older adults. This understanding is the key to effectively implementing a surveillance system and screening programs to alleviate the burden of CKD in Saudi Arabia. One of the major strengths of our study is its comprehensive data collection process. We gathered data from across the country, covering various individuals. The data were collected nationwide from 42 branches of Alborg laboratories in 13 regions, indicating that the study's findings likely represent the entire Saudi Arabian population. Region-specific interventions are recommended, focusing on areas such as Makkah and Jazan, where CKD prevalence is notably higher. Primary prevention strategies should include public health campaigns promoting awareness about CKD risk factors, such as diabetes and hypertension, and encouraging routine health check-ups to detect CKD at earlier stages. Lastly, longitudinal data collection and registry systems should be enhanced to monitor CKD trends and evaluate the effectiveness of interventions, ensuring evidence-based policymaking and sustainable healthcare practices.
Like any research, our study also has limitations. We acknowledge the potential for incomplete or inconsistent data collection and the possibility of missing data. We also note that the study did not evaluate certain factors, such as the cause, genetic predisposition, environmental toxins, and associated comorbid conditions and their duration. The definition of CKD in the study was limited to decreased eGFR without considering albuminuria status or structural damage. Moreover, we might have selection bias in our study, where we failed to include some participants’ data from certain areas in our study such as Northern border area and Aljouf during the entire recruitment period. Finally, the study's cross-sectional design restricts its ability to assess causality. These limitations are important to consider when interpreting the findings of our study.




Comments (0)