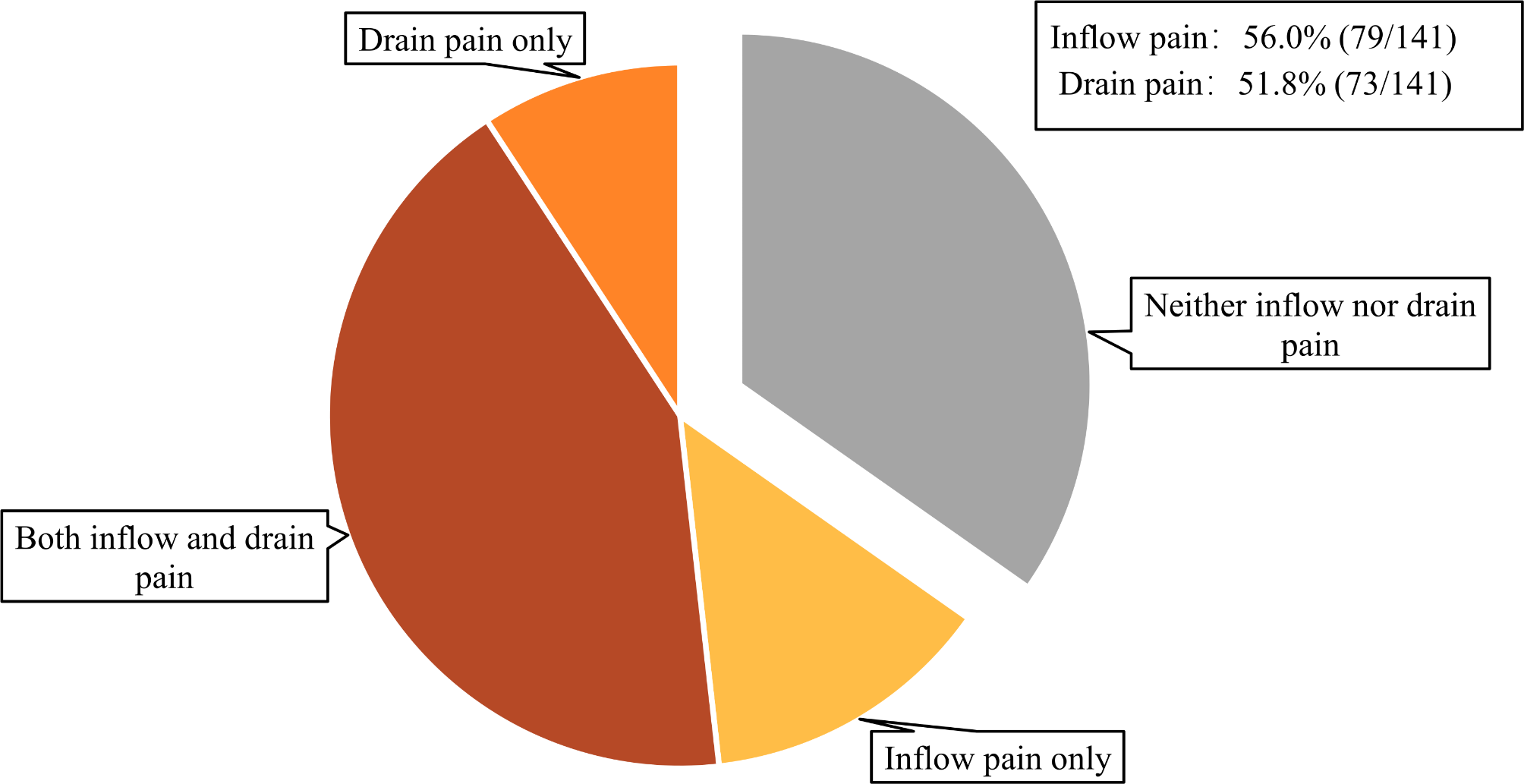
This study revealed that the incidence of inflow pain one week after catheter implantation was 56.0%, while drain pain occurred in 51.8% of cases. Moreover, 39.2% of patients experienced severe inflow pain, and 30.1% reported severe drain pain within the first week postoperatively. Notably, 17.3% and 19.5% of patients still had inflow pain and drain pain, respectively, at 3 months postoperatively.
Previous studies have reported varying incidence rates of inflow and drain pain. Inflow pain can occur in 13-33% of patients [8], while drain pain is reported in 19.6-36.3% of cases [9, 10]. Discrepancies in pain incidence across studies may be due to differences in study populations, dialysis duration, sample sizes, and data collection methods. Our study uniquely reported the incidence rates within the first week and at subsequent 3 months. The results revealed that, compared to long-term PD patients in other studies, incident PD patients experienced significantly higher rates of inflow pain and drain pain, reaching 56.0% and 51.8%, respectively. These incidences decreased significantly at 1 month postoperative, which is consistent with previous research and clinical experience [5, 8, 9]. In addition, 39.2% and 30.1% of patients reported severe inflow and drain pain, respectively, within the first week postoperative, highlighting their significant impact on patients’ quality of life. This underscores the critical need for management of these issues in clinical practice for incident PD patients.
Patients commonly alleviate pain by adjusting the infusion rate or halting drainage of peritoneal dialysate, practices frequently mentioned in prior research [11]. Inflow pain typically results from rapid peritoneal fluid impact on the bladder or rectum, whereas drain pain arises from visceral structures migrating towards the catheter tip, exerting pressure on sensitive parietal tissue [11, 16]. Hence, the rate of dialysate exchange emerges as a critical factor influencing pain levels, consistent with our finding. Additionally, catheter positioning plays an important role, with patients able to alleviate pain by adjusting their posture to potentially relieve discomfort related to catheter placement.
Age, gender, and the method of PD catheter implantation were identified as independent factors influencing pain among PD patients within the first week postoperatively. However, by the 1-month postoperative, gender and a history of previous abdominal surgery were significant factors affecting pain levels. It’s worth noting that the factors influencing pain within the first week postoperative differed significantly from those at 1 month and 3 months postoperative. This disparity may be attributed to the acute stress experienced by patients immediately after surgery and the relatively smaller sample size due to the significant decrease in pain incidence after the first month postoperative.
Younger patients were more likely to experience inflow or drain pain within 1-week postoperative, with age identified as an independent risk factor during this early period. Lautenbacher et al. found that pain threshold elevated with increasing age, resulting in patients being less sensitive to pain [17]. Similarly, Tighe et al. noted that older patients tend to have lower immediate postoperative pain scores, but slower pain resolution over time [18], which could account for the lack of age-related effects observed at 1 month and 3 months postoperatively in our findings. Furthermore, gender was consistently associated with inflow or drain pain across different time points. It also have been revealed that higher prevalence of pain among women across various pain types, including cancer pain, postoperative pain, low back pain, and muscular pain [19]. This gender disparity in pain experience may be influenced by factors such as sex hormones, opioid receptors in the brain, and psycho-social elements.
Our study found that among patients who did not experience inflow or drain pain, the proportion of diabetics was higher. This finding is consistent with a study on postoperative pain after colorectal surgery, where diabetes mellitus was independently linked to reduced pain. The authors proposed that diminished sensory input due to diabetic neuropathy could be a contributing factor [20, 21]. These findings underscore the importance of preoperative assessment and proactive pain management during the perioperative period of peritoneal dialysis, particularly in young female patients and those without a history of diabetes mellitus.
In constipated patients, surgical procedures may be influenced by bowel distention, potentially resulting in suboptimal catheter placement within the vesicouterine pouch or rectovesical pouch of the pelvis. This could cause reduced patient sensation during dialysate inflow, possibly explaining why constipation was associated with lower occurrence of pain at 1 week postoperatively. Further, varying degrees of peritoneal adhesions and fibrosis often follow abdominopelvic surgery [22]. As a result, patients without prior abdominal surgery may have weaker intra-abdominal tissues and more sensitive nerves, rendering them more susceptible to pain. This is supported by our finding that a history of previous surgery was protective against inflow or drain pain at 1-month postoperatively. A novel observation from our study is that the pneumoperitoneum needle method of catheter implantation is a risk factor for inflow or drain pain within the first week postoperatively, which has not been reported previously. It is speculated that in this method, lacking direct visualization of the omentum during PD catheter placement, may result in a relatively higher incidence of catheter dysfunction and experience more intense inflow or drain pain, compared to the open surgical approach. This also suggests that, although the pneumoperitoneum needle method is generally advantageous for most patients, offering shorter procedure times and less trauma, young patients with active omentum should approach this modality with caution. However, this hypothesis requires further investigation to be validated. Due to the limitation of blind implantation, we suggest using a rigid guidewire to guide the catheter into the intraperitoneal cavity by closely adhering it to the anterior abdominal wall. The effectiveness of this method, however, requires further observation and study.
This study has several limitations that should be acknowledged. Firstly, it is a single-center observational study with a small sample size, potentially limiting its statistical validity and the generalizability of the conclusions. Secondly, while previous research suggested that catheter position could significantly impact pain [16], this aspect was not further analyzed due to the subjective nature of depth placement during PD catheter implantation and the lack of objective data recording. Thirdly, this study only tracked patients’ pain for up to 3 months postoperatively and did not differentiate between inflow pain and drain pain for long-term risk factors analysis in the PD population. Fourth, in the previous study design, we only focus primarily on patients’ pain at the start and end of treatment, and did not pay much attention to patients’ pain in the APD intertreatment phase. To further explore this information, we followed up patients who reported pain on APD treatment and found that none of them experienced reportable inflow or outflow pain during the tidal cycle. Nevertheless, we recognize that this conclusion may be influenced by recall bias. Last, compared to the open surgical and pneumoperitoneum needle methods of PD catheter implantation, laparoscopic implantation, which allows for direct visualization, adhesiolysis, or omentectomy during surgery, may reduce the incidence of inflow and drain pain [23, 24]. However, as laparoscopic implantation was not utilized in our center, we were unable to analyze its impact on postoperative inflow and drain pain in this study. These limitations underscore the necessity for larger, multicenter studies with objective measures of catheter placement and long-term follow-up to provide more robust insights into pain management in PD patients.




Comments (0)