
Remember me



Multisystem Inflammatory Syndrome (MIS) is a rare but severe condition that emerged during the coronavirus disease 2019 (COVID-19) pandemic, primarily affecting children (MIS-C) and, to a lesser extent, adults (MIS-A) [1, 2]. It typically presents 4–12 weeks following severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) infection, and more rarely other bacterial or viral diseases, and is characterized by widespread systemic inflammation that can impact multiple organ systems [2, 3]. Among the most serious complications of MIS is cardiac involvement, particularly the inflammation of the myocardium (myocarditis) and the pericardium (pericarditis) with significant morbidity and, in some cases, mortality (Fig. 1) [2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17]. Despite the clinical relevance, the pathogenesis of cardiac involvement in MIS is poorly understood, and evidence supporting clinical management is scarce. This review article aims to provide an in-depth exploration of the myocardial and pericardial involvement in MIS, discussing the possible pathophysiology, clinical features, and the current knowledge gaps in the field.
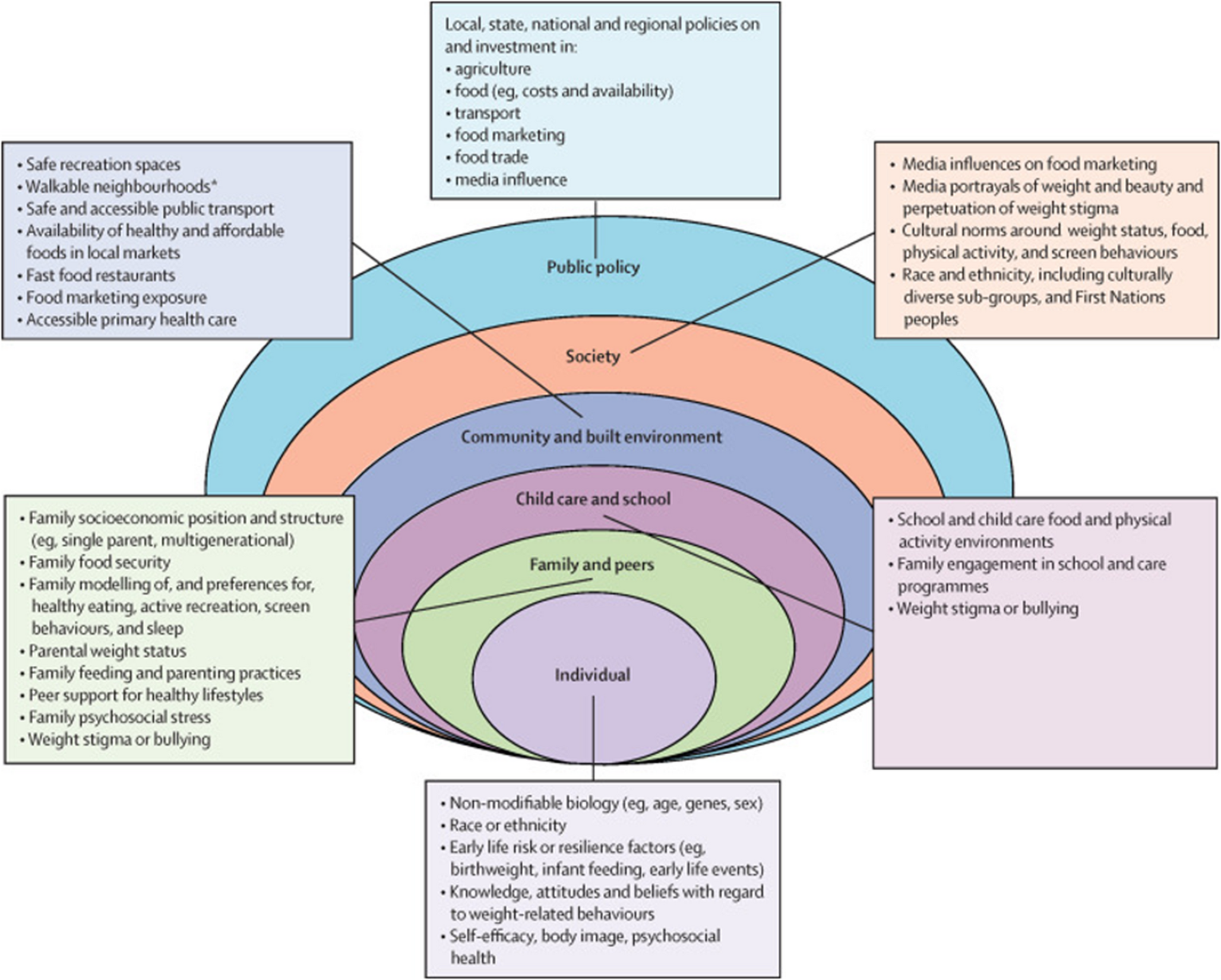
Fig. 1
Myocardial and Pericardial Manifestations of Multisystemic Inflammatory Syndrome with Cardiac Involvement. The figure illustrates the clinical manifestations, laboratory and imaging (both at echocardiography and cardiovascular magnetic resonance) findings of Multisystem Inflammatory Syndrome (MIS) with myocardial and pericardial involvement. The figure summarizes the main pathophysiological mechanisms leading to the cytokine storm underlying the cardiac manifestations of this syndrome. Figure created with BioRender.com. Abbrev: AV: atrio-ventricular; ECG: electrocardiogram; CMR: cardiovascular magnetic resonance; CRP: C-reactive protein; echo: echocardiogram; ESR: erythrocyte sedimentation rate; IL: interleukin; LGE: late gadolinium enhancement; LV: left ventricular; NLRP3 inflammasome: pyrin domain-containing-3 inflammasome; NT-proBNP: N- terminal pro-b-type natriuretic peptide; RMWA: regional wall motion abnormality; SARS-CoV-2: severe acute respiratory syndrome coronavirus 2; STIR: short-tau inversion recovery; VES:; VT: ventricular tachycardia; VF: ventricular fibrillation
Epidemiology and PathophysiologyThe epidemiology of MIS is still unclear due to a lack of distinctive clinical features and easy-to-use definition. As such, the incidence, likely underestimated, remains relatively low compared to the total number of SARS-CoV-2 infections. In children, the highest incidence of this condition was documented among previously healthy individuals aged 5–14 years. A multicentre study by Feldstein and co-authors reported that patients diagnosed with MIS-C were more likely to be younger (mean age of 8.9 years, interquartile range [IQR] of 4.7 to 13.2 vs 11.7 IQR [1.2–16.6]) compared to patients with COVID-19, with a predominance of males affected (62% vs 38% of females) [17]. Moreover, MIS-C was more commonly observed among Black non-Hispanic and South Asian populations, though the reasons for this racial disparity are not fully understood [1, 17, 18]. Similarly, in the largest cohort of MIS-A by Patel et al. involving 221 subjects, patients affected were relatively young (median age 21 years), with no underlying comorbidity in most cases [5]. Moreover, males were predominantly affected (70% vs 30% of females) with a large prevalence of non-Hispanic Black individuals (36% of the overall population) as reported in children [5].
The pathophysiological mechanisms underlying MIS remain unknown, but it is believed to be a post-infectious immune-mediated condition. A hyperinflammatory state characterized by macrophage activation and elevated levels of pro-inflammatory cytokines, such as Interleukin-1β (IL-1β), IL-1α IL-6, and tumor necrosis factor (TNF) leads to a "cytokine storm" that in turn causes widespread tissue damage and amplifies the inflammatory response [2, 19]. In particular, the signaling of IL-1 family of cytokines plays a pivotal role in the pathogenesis of this syndrome. The IL-1 has two active forms: IL-1α and IL-1β.The latter is activated by inflammatory cells from its precursor, the pro-IL-1β, by caspase-1 enzymes which are triggered by the NLRP3 inflammasome [20,21,22,23,24].In MIS-C, the NLRP3 inflammasome pathway is probably activated by danger-associated molecular patterns (DAMPs), as elevated transcription products are observed during the acute phase of the disease [25]. Given the central role of NLRP3/IL-1β in cardiovascular diseases, it is likely that the NLRP3 inflammasome and IL-1β signalling also contribute to the cardiac involvement in MIS-A. The release of DAMPs and pathogen-associated molecular patterns (PAMPs) further activates innate immune cells, including macrophages and dendritic cells, leading to the secretion of additional pro-inflammatory cytokines like IL-6, which further amplify the inflammatory response and activate the adaptive immune response by stimulating T-cell development and antibody production to combat the viral infection [2, 26]. However, elevated IL-6 levels are also linked to immune dysregulation in pediatric illnesses, such as Kawasaki Disease (KD), as well as in COVID-19, where high IL-6 levels are associated with worse clinical outcomes [27, 28]. Thus, cytokines and ensuing activation of the adaptive immune response may in some cases trigger the immune-mediated processes further contributing to disease progression. Other molecular mechanisms involved in the pathogenesis of the disease include adaptative immune response dysregulation and T lymphocyte cell activation through epitope cross-reactivity with self-antigens and immune complexes formation [2]. Immunophenotyping of peripheral blood cells in patients with MIS-C showed characteristic changes in the proportions and functions of naïve CD4 + and CD8 + cytotoxic T cell counts, with significantly reduced levels of CD8 + , as were the ratios of monocyte and natural killer (NK) cell ratios [29, 30]. On the other hand, it has been documented a neutrophil and CD16 + monocyte increased activation and a high expression of migration proteins (ICAM-1), all indicating increased flow of myeloid cells to the periphery [31]. The reduced levels of circulating CD8 + and NK cells, together with enhanced activation of myeloid cells in the periphery contribute to maintaining the multiorgan systemic inflammation underlying MIS [29]. Cross-reactivity of viral epitopes with tissue-specific self-antigen or virus-encoded superantigens activating the CD4 + T lymphocytes have been also hypothesized as potential molecular pathways activated in cases of T-cell mediated myocarditis documented in adults [12]. Furthermore, circulating immunocomplexes of spike proteins of the virus have been isolated in patients affected by MIS-C, suggesting also a possible “superantigen-like response” where viral epitopes may elicit a non-specific polyclonal T cell activation and a massive cytokine release responsible for the hyperinflammatory state [32,33,34].
The reason for the higher prevalence of the disease among children is not completely understood. A stronger predisposition to an enhanced activation of the innate and adaptative immune response following the COVID-19 infection in children may lead to a more efficient clearance of the infection but a higher predisposition to develop MIS [5]. On the other hand, adults are more prone to delayed clearance of the virus due to immunosenescence and immune dysregulation, which can be responsible for more severe COVID-19-related symptoms rather than MIS. Furthermore, in older adults, the clinical presentation of MIS may be more complex due to coexisting autoinflammatory or severe comorbidities that make the diagnosis particularly challenging.
Clinical Features and Differential Diagnosis of MISExtra-cardiac clinical features of MIS are remarkably heterogeneous and include persistent fever associated with signs of mucocutaneous involvement (annular macular rash or non-purulent conjunctivitis), gastrointestinal symptoms (vomiting, diarrhea), hematological (e.g. neutrophilia, but also lymphopenia and thrombocytopenia) and coagulation disorders (arterial and venous thrombosis). Moreover, patients with MIS typically present very high levels of circulating inflammatory biomarkers (C-reactive protein [CRP], IL-6, ferritin), generally higher compared to those found in patients with COVID-19 without MIS [17]. The above-mentioned clinical signatures are not exclusively associated with MIS but significantly overlap those of other pro-inflammatory conditions (e.g. Kawasaki disease [KD], Adult-Onset Still’s Disease [AOSD], the macrophage activation syndrome [MAS], viral myocarditis), thus making the diagnosis particularly challenging, especially in children (Table 1). Therefore, the Brighton Collaboration MIS-C Working Group proposed a case definition of MIS-C/A, which included the evidence of fever (subjective fever or documented fever [≥ 38.0 C]) and ≥ 2 clinical findings of systemic inflammation (mucocutaneous, gastrointestinal, neurological symptoms, hypotension/shock) (Table 2). Also, patients with MIS should have: (i) evidence of current or previous (within 12 weeks) SARS-CoV-2 infection; and (ii) signs of significant systemic inflammation and/or coagulopathy [1]. Signs and symptoms of cardiac involvement are considered under the primary diagnostic criteria, according to large population cohort studies reporting a predominant cardiovascular involvement among the distinctive signatures of the disease [5, 17]. These include evidence of myocardial and pericardial involvement (myocarditis or left ventricular systolic dysfunction [LVEF < 50%] and pericarditis), as well as coronary artery dilatation/aneurysm, more frequently observed in children, and brady- or tachi-arrhythmia (e.g. 2nd/3rd degree atrioventricular block, or ventricular tachycardia).
Table 1 Note: This data is MandatoryTable 2 Centers for Disease Control and Prevention Diagnostic Criteria of Multisystem Inflammatory Syndrome in Adults (MIS-A/C)MIS can also mimic the clinical manifestations of a multi-organ involvement during the SARS-CoV-2 infection. However, compared to COVID-19 patients, individuals with MIS present more frequently with cardiovascular but not respiratory involvement, and with mucocutaneous manifestations of the disease [17]. Moreover, patients with MIS present more often neutrophilia and thrombocytopenia than lymphocytopenia and have higher levels of pro-inflammatory biomarkers (e.g. CRP and IL-6) within 48 h from admission compared to patients with COVID-19 [17].
Cardiac Involvement in MISCardiac involvement in MIS is common but heterogeneous and can range from mild myocardial dysfunction to severe, life-threatening conditions such as acute heart failure, cardiogenic shock (CS) and life-threatening arrhythmias. The cardiovascular system is more frequently involved in MIS-A than MIS-C, with a higher incidence of cardiac dysfunction documented in adults compared to children (54% vs 29%) [2, 16]. Moreover, in young adults it is described a higher rate of severe complications related to the cardiac involvement, with a larger proportion of deaths compared to what observed in patients with MIS-C (7% vs 1%) [5]. Among the cardiac manifestations of the disease, myocarditis and/or pericarditis are highly prevalent. A systematic review by Junior et al. reported a combined incidence of myopericarditis of 34% in patients with MIS-C [35]. Similarly, Patel et al. reported an incidence of myocarditis of 30% and of pericardial effusion of 25% in MIS-A patients [5]. Myocarditis may lead to various degrees of cardiac dysfunction [2,3,4,5,6,7,8,9,10,11,12,13,14]. Patients affected usually present with high levels of cardiac biomarkers (Troponin I or T, brain natriuretic peptide [BNP] or N-terminal pro B-type natriuretic peptide [NT-proBNP]), electrocardiographic (EKG) changes consistent with myocarditis (abnormal ST segments or low voltage QRS in the presence of edema), ischemia (abnormal ST segments, T wave inversion) or ventricular tachyarrhythmia (e.g. ventricular tachycardia [VT] or ventricular fibrillation [VF]). Bradyarrhythmia (atrioventricular or intraventricular conduction delay) and supra-ventricular tachyarrhythmias (atrial fibrillation or atrial flutter) are less frequent, but still possible manifestations accompanying the myocardial involvement of MIS-A [2]. Cardiac imaging modalities, such as transthoracic echocardiography and cardiac magnetic resonance (CMR) are the cornerstone diagnostic techniques to demonstrate myocardial damage [2]. In particular, transthoracic echocardiography can identify the presence and severity of left ventricular or biventricular systolic dysfunction (also assessed through ventricular myocardial speckle strain imaging), with or without regional wall motion abnormalities as well as diastolic dysfunction or less frequent complications such as valvulopathies (e.g. mitral regurgitation) [2]. CMR can provide more accurate quantification of cardiac volumes and function and pivotal diagnostic information on myocardial damage through its ability of tissue characterization. Previous studies showed that evidence of myocarditis according to the updated Lake Louise criteria can be found in up to 35% of patients with MIS-C, including the evidence of T2-based markers for myocardial edema (on short-tau inversion recovery [STIR] or T2 mapping sequences) and a T1-based markers for associated myocardial injury (late gadolinium enhancement [LGE], increased native myocardial T1 mapping and/or extracellular volume [ECV] values) [36,37,38]. An abundance of data from case series supports these findings also in adults [5, 7,8,
Comments (0)