The results presented in this manuscript show that robustly optimized IMPT can be used for high-dose (70–74 Gy [RBE]) treatment of skull base chordomas and chondrosarcomas with good CTV coverage (97.66–98.00%), even in the presence of implants, while sparing the adjacent dose-sensitive structures with little plan adaptation and necessary position-evaluation cone-beam CT, weekly CT scans, and daily kV-kV imaging.
Although gross total resection is considered the mainstay of treatment for chordomas and chondrosarcomas, for lesions localized in the skull base this is not possible without major morbidity for most patients. Dose-escalated radiotherapy is therefore often used as an adjuvant or alternative treatment to optimize local tumor control with good results, particularly for radiotherapy delivered with protons [4,5,6, 8, 13,14,15,16,17,18,19,20,21]. Results of one of the largest studies on long-term outcomes of proton therapy in 151 chordomas and 71 chondrosarcomas of the skull base have shown that long-term local tumor control can be achieved regardless of the level of resection [6]. In a subset of patients, the biological behavior of the tumor is such that radiotherapy can be reserved for treating tumor recurrence.
A potential downside of radiation therapy in general that has to be considered is its sensitivity to system setup and patient positioning uncertainties. In photon radiotherapy these uncertainties are accounted for by adding an extra margin around the clinical target volume to create the planning target volume (PTV) [8, 21]. Contrary to photon beams, proton beams are more sensitive to the presence of heterogeneities along their path, which can cause dose perturbations and formation of so-called hot spots and cold spots within and close to the target. This is of utmost importance, especially when high doses are administered in a location with nearby critical structures, such as the skull base. The PTV approach is not able to account for all these heterogeneities, making it a not so ideal method for proton therapy [8, 22]. However, Monte Carlo simulation-based robust optimization, which re-evaluates and re-calculates treatment plan scenarios for different setups for each proton beam, accounts better for uncertainties in IMPT. Although robust optimization is more time consuming compared to conventional PTV-based optimization, it is less sensitive to uncertainties, making it superior to conventional PTV-based optimization [23,24,25]. Additionally, for smaller CTVs, as often encountered in the skull base region, worst-case-scenario-based robust optimization proved to be better than conventional optimization [14].
The frequent presence of titanium implants in the vicinity of the irradiated tumor volume renders treatment planning more difficult. The high-density titanium implants cause hardening of the CT X‑rays, thus resulting in image artifacts that often make accurate target delineation difficult. These artifacts, along with the increased medium heterogeneity caused by the implant, further interfere with the accuracy of dose calculation, which could result in tumor underdosage and formation of the previously mentioned hot spots and cold spots. To avoid creation of hot spots, Rutz et al. administrated a reduced dose per fraction (1.8 Gy [RBE]) and reported a positive correlation between the presence of metallic implants and local failure in extracranial chordoma patients treated with proton therapy [26]. DeLaney et al. reported a slightly lower local failure rate (35 vs. 38%), proposing that the location of the tumor and the level of resection have an impact on the local failure rate [27]. Staab et al. reported a 30% 5‑year local control rate in skull base, spinal, and sacral chordoma patients with metallic implants treated with proton therapy [28]. Difficulties with artifacts, dose calculations, and beam positioning that arise are a main reason why some centers opt not to perform proton therapy in patients with implants [29]. Nevertheless, in our study, 4 patients with titanium implants were successfully treated with IMPT. In our center, the main strategy for administrating proton therapy in such cases is consultation with the treating neurosurgeons both prior to and after the surgery in order to align the position of the surgical implant and clinical target volume for the optimal proton treatment plan.
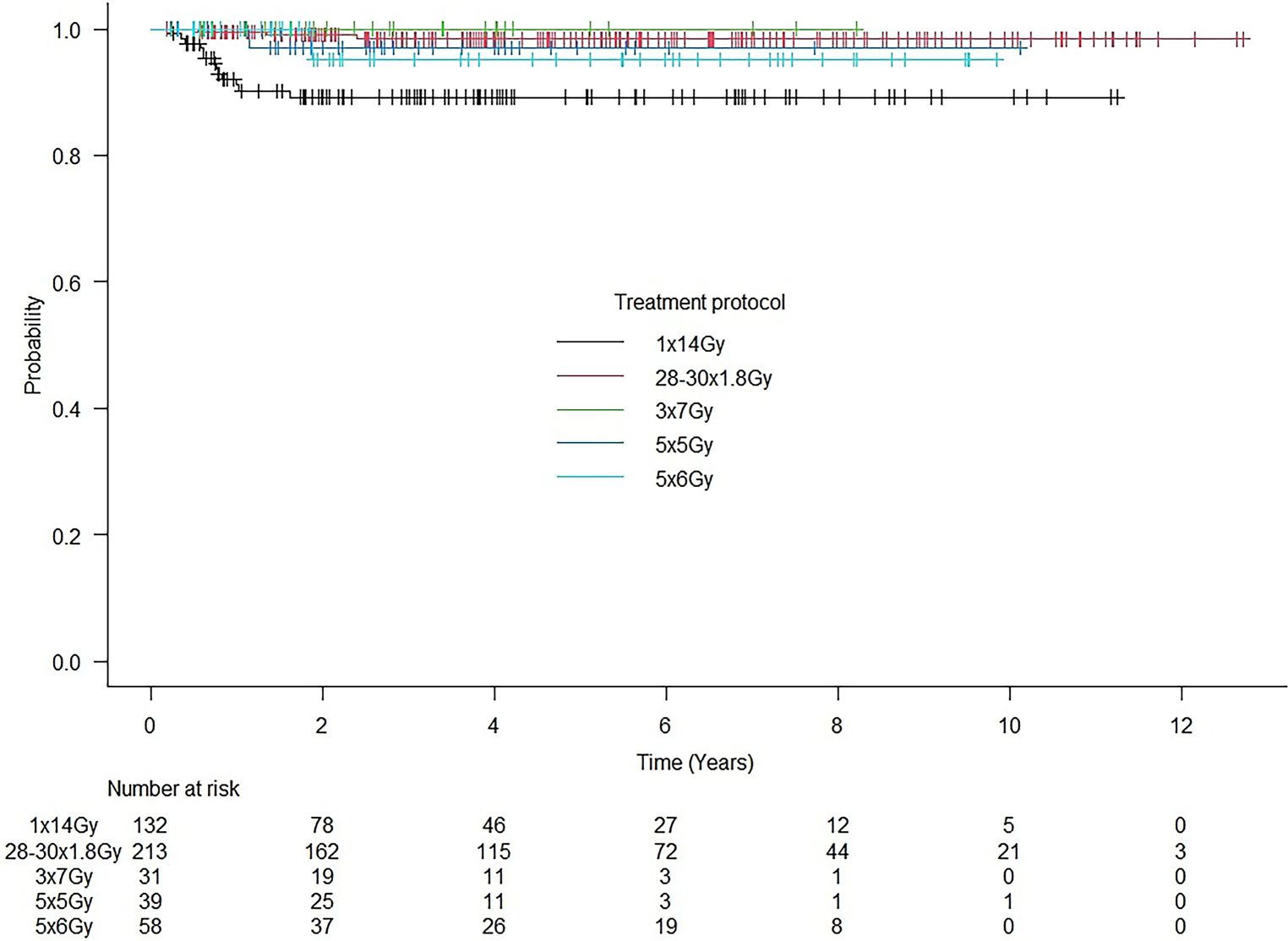
With the low radiosensitivity of chordomas and chondrosarcomas, administration of the necessary high doses in the vicinity of critical organs, especially in the complexly structured area of the skull base, can be challenging. Unlike photons which continuously deposit energy along their trajectory, protons have a rapid dose fall-off at the end of their trajectory, thus allowing locally high dose deposition while sparing the adjacent dose-sensitive organs and rendering proton therapy a more favorable treatment modality. Reported 5‑year local control rates are in favor of skull base chordoma and chondrosarcoma patients treated with protons compared to those treated with photons—81 and 65.3% in chordomas and 94 and 88.1% in chondrosarcomas, respectively [30, 31]. Despite being more sensitive to uncertainties as compared to photon therapy, as mentioned above, proton therapy-induced toxicities are acceptable. Ares C. et al. reported grade 3 toxicities in 3 patients (neuropathy, central nervous system necrosis) and grade 4 toxicity in only 1 patient (neuropathy) among 64 patients during a mean follow-up period of 38 months [30]. Mattke M. et al. reported up to grade 2 temporal lobe toxicity in 44 out of 147 skull base chordoma patients treated with proton therapy, out of whom 20 patients had temporal lobe necrosis [11]. Other commonly reported early toxicities such as hearing impairment, dry eye, vision impairment, dry mouth, and radiation dermatitis were also seen among the patient group presented in this study (Table 3; [7, 32,33,34,35]). Most of these toxicities spontaneously disappeared 3 months after treatment.
Our results, as well as those of previously published studies, demonstrate that robustly optimized IMPT is feasible for lesions located in the head and neck region with low-grade toxicities [10, 11, 15, 24, 33]. Long-term sequelae are currently actively monitored and recorded for future treatment adaptation and improvement.

Comments (0)