Sarcomas with KAT6B/A::KANSL1 fusion were first described in one retroperitoneal and one uterine tumor originally diagnosed as leiomyoma, followed shortly after by a tumor initially diagnosed as uterine leiomyosarcoma [12,13,14]. However, the chromosomal rearrangements at specific loci on chromosome 10q and 17q had been sporadically reported in smooth muscle tumors before [22,23,24]. In 2022, Agaimy et al. described a series of 13 uterine tumors with KAT6B/A::KANSL1 fusion and suggested, for the first time, that these cases represent a distinct entity [9]. In 2023, Trecourt et al. reported a series of further 12 patients [11]. In both studies, tumors with these fusions mostly showed overlapping features between leiomyoma and LG-ESS, but a few tumors with high-grade features were also present [9, 11]. In the first study, the authors described 13 cases, of which 10 were originally diagnosed as LG-ESS, and one case each was diagnosed as LMS, leiomyoma, and undifferentiated uterine sarcoma [9]. The reported assigned diagnoses have also changed over time during the diagnostic process, based on molecular findings and observations in the recurrent tumors, and included also uterine tumor resembling ovarian sex cord tumor, cellular leiomyoma, and myxoid leiomyosarcoma. Apart from one tumor with high-grade features, all other tumors showed bland morphology and were well circumscribed in most cases, but despite this commonly behaved in malignant fashion. Three patients died of the disease, three were alive with disease, five showed no evidence of disease, and in two recent cases, the follow-up was not available. In the second study on 16 tumors from 12 patients, the initial diagnosis was leiomyoma in 6/16 tumors, ESN or endometrial stromal tumor in 4/16 cases, LG-ESS in 4/16 cases, and intravenous leiomyomatosis in 2/16 cases [11]. The follow-up was available for 9 patients, of whom 3 relapsed and 6 were without evidence of disease. In our study, 5/8 patients showed recurrent disease, two of which died of disease and three were alive with disease.
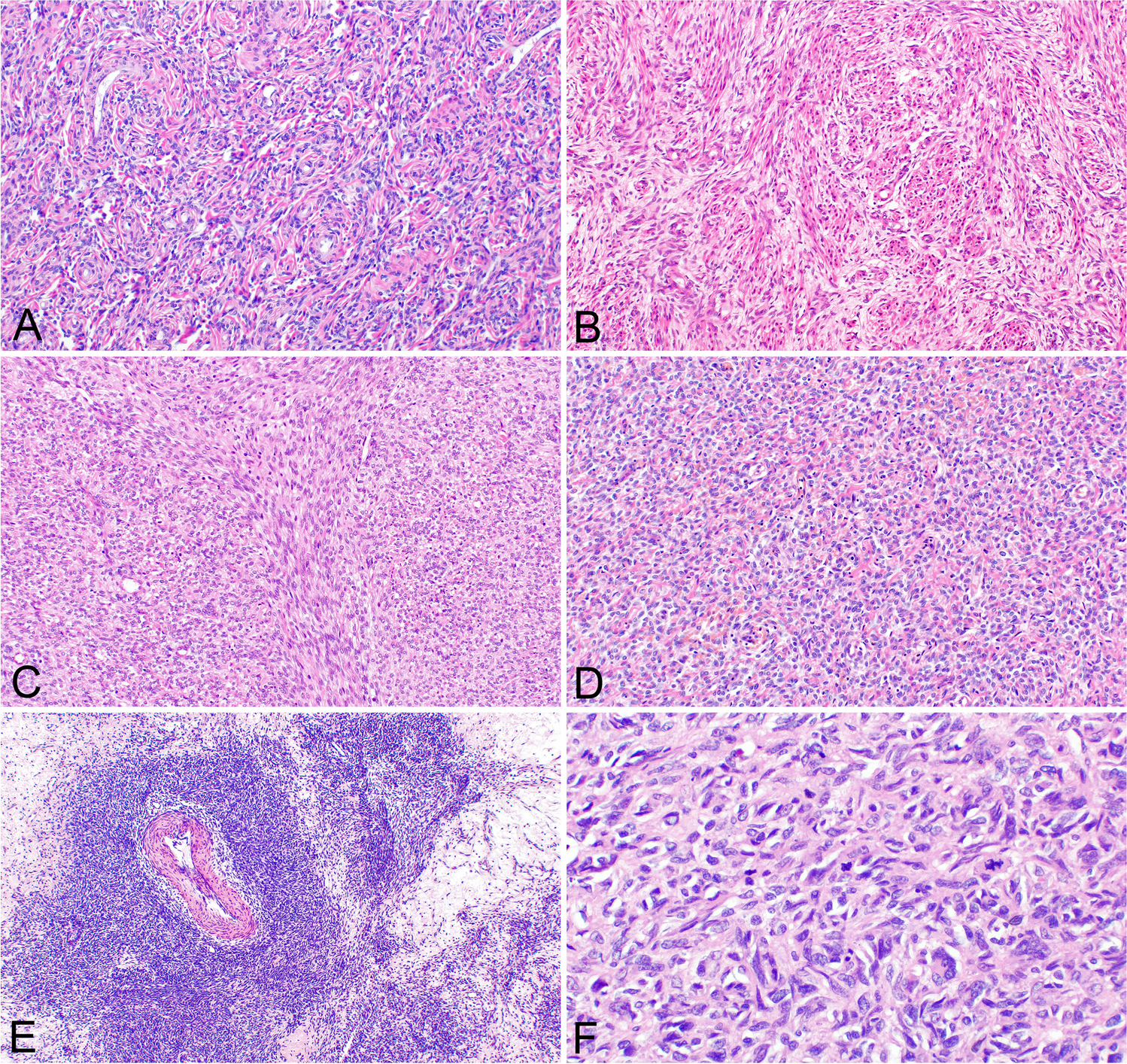
The differential diagnosis of sarcomas with KAT6B/A::KANSL1 fusion showing low-grade features mainly includes tumors with endometrial stromal or smooth muscle differentiation. Most cases in the published studies were originally diagnosed as LG-ESS, but given the sharp demarcation of some tumors, they can also be misdiagnosed as endometrial stromal nodules. According to current knowledge, reliably rendering the correct diagnosis based only on morphological and immunohistochemical features is not possible. The morphology of sarcomas with KAT6B/A::KANSL1 fusion is variable, but almost all cases exhibited some features suggestive of endometrial stromal differentiation (fibroblastic or fibromyxoid) or hybrid features between endometrial stromal and smooth muscle differentiation. Rarely, only features suggestive of smooth muscle differentiation can be found. Moreover, rare tumors can show high-grade features (6% of all reported cases, including ours), and these cannot be differentiated from high-grade endometrial stromal sarcoma or undifferentiated uterine sarcoma based on morphological features alone. Concerning the morphological features of tumors with low-grade appearance, the cells can be ovoid, spindled, or both, with usually round or oval, and rarely spindle-shaped nuclei. Mitotic activity is variable and can exceed 20 mitoses/10 HPF, but mostly is up to 5/10 HPF. Nuclear atypia is mild or moderate. The architecture is typically heterogeneous, including solid, nested, fascicular, and storiform patterns, and in some cases even schwannoma-like or sex cord-like features. The whorling pattern which is characteristic for fibromyxoid LG-ESS is commonly present, as are hyaline collagen deposits. The vasculature typically consists of arterioliform vessels typical for endometrial stromal tumors, but larger, thick-walled vessels are also commonly found. Pericytoma-like vasculature has been reported as a common finding, but in our study, it was present in only two cases. The demarcation from the surrounding myometrium is typically sharp, but the infiltrative pattern and tongue-like invasion characteristic of LG-ESS can also be seen.
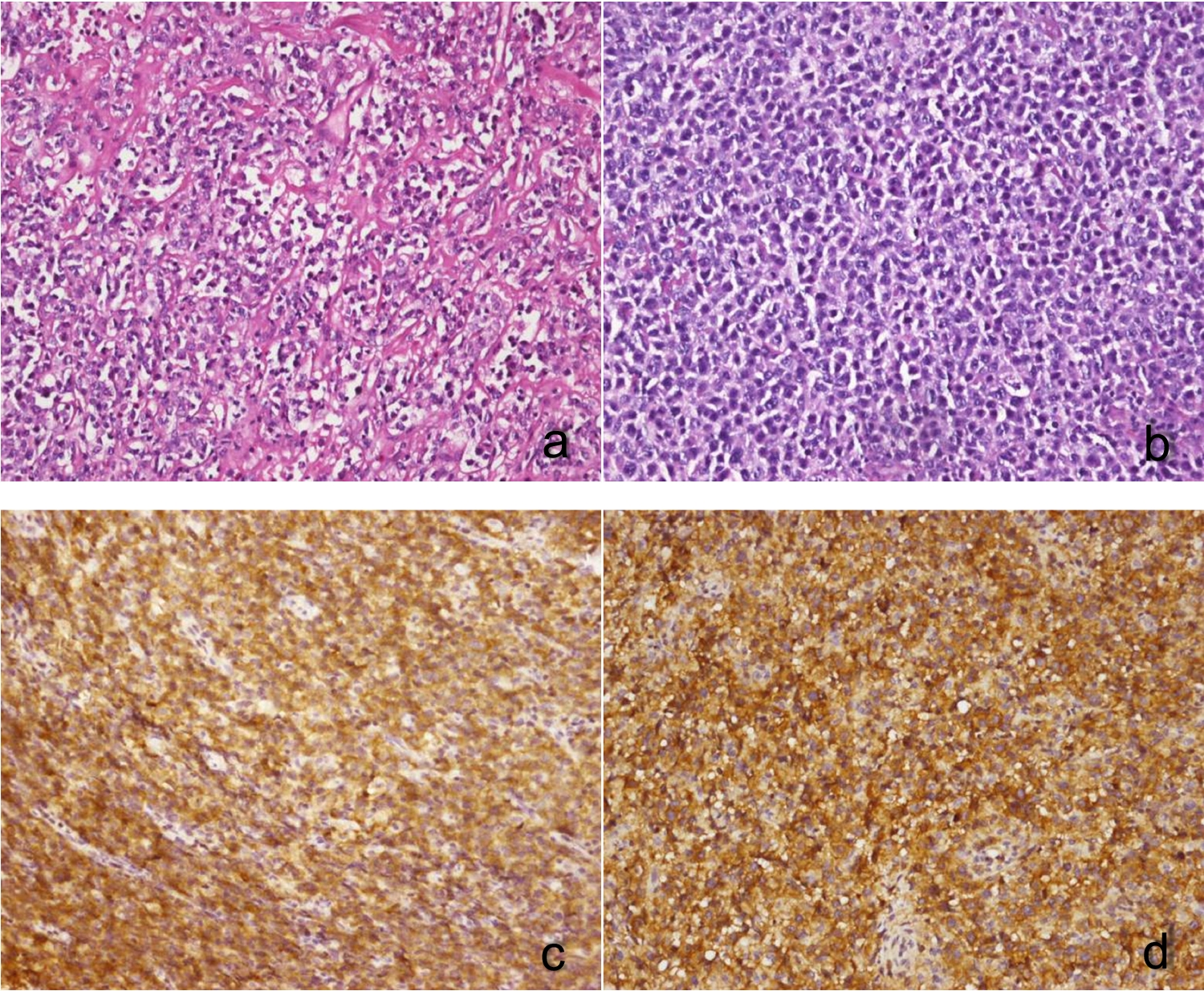
Immunohistochemically, the combined data from our and both previously published studies suggest that most tumors express estrogen (91%) and progesterone receptors (89%) and show variable expression of smooth muscle and “endometrial stromal” markers [9, 11]. The expression of smooth muscle markers seems to be limited in both the spectrum of markers expressed and their extent of positivity. The most commonly expressed marker was smooth muscle actin (88%). The expression of transgelin and calponin was found in 56% cases, desmin in 39% cases, and caldesmon in 25% cases. The tumors showed common expression of endometrial stromal markers, such as CD10 (92%) and IFITM1 (73%). Nevertheless, these markers are not specific and CD10 especially is typically expressed not only in LG-ESS/ESN, but also in a subset of leiomyomas, especially the cellular variant [25]. The expression of WT1 seems to be at most focal and weak in most sarcomas with KAT6B/A::KANSL1 fusion, and 50% of the analyzed cases were entirely negative, which would be unusual for LG-ESS. According to current knowledge, sarcomas with KAT6B/A::KANSL1 fusion cannot be diagnosed based only on morphological and immunohistochemical features. Tumors with features suggestive of this diagnosis, particularly including overlapping features between endometrial stromal and smooth-muscle differentiation, should undergo molecular testing, preferably by NGS, which also allows the assessment of other recurrent molecular alterations typical for some other entities entering the differential diagnosis. Alternatively, our study showed that the KAT6B/A::KANSL1 fusion can be reliably detected by FISH analysis using an appropriate pair of fusion probes.
One of the previous studies proposed a diagnostic algorithm for these tumors, incorporating clinical features (perimenopausal women and uterine corpus location), microscopic and immunohistochemical features, and molecular findings [11]. Concerning microscopy, the authors emphasized some relevant features such as the presence of hybrid morphology of leiomyoma and LG-ESS or ESN, whorling pattern, arterioliform vasculature, central hyalinized vessels, and spindled or ovoid cells with mild to moderate atypia and few mitoses. Immunohistochemically, the tumors are supposed to be characterized by estrogen and progesterone receptor expression, and variable expression of smooth muscle markers and endometrial stromal markers, such as CD10 and IFITM1. However, applying both the clinical and pathological features, our cases would not entirely fit based on this suggested algorithm.
The potential additional molecular alterations beyond KAT6/B::KANSL1 gene fusion in these tumors have not been widely investigated. In one previous study, the authors did not detect any pathogenic variants in their cohort [11]. However, this might be attributed to the imperfect method used in this study for generating those results, as their mutation analysis was conducted using cDNA (synthesized from RNA). This approach is not optimal for mutation detection, especially for FFPE samples, as it often results in insufficient coverage, particularly for genes with low transcript levels [26]. In another recent study, the authors focused on methylation profiling and copy number alterations in 18 sarcomas with KAT6B/A::KANSL1 fusion [10]. Their results showed that aggressive tumors have a different methylation profile, but also harbor various copy number alterations, including deletions of the CDKN2A/B and NF1 loci. In our study, we detected additional pathogenic or likely pathogenic mutations in all 5 aggressive tumors, including mutations in FANCD2, RB1, PTEN, ATM, TP53, NF1, TSC1, CREBBP, or PDGFRB genes. All these genes are involved in complex signaling pathways that regulate DNA repair, cell cycle control, and cell proliferation. Moreover, one patient without evidence of disease had a mutation in ERCC3 gene, which is involved in DNA damage repair, and one patient also with no evidence of disease had no detected mutations. All the detected mutations can also be observed in tumors with smooth muscle and endometrial stromal differentiation and are not specific for tumors with the KAT6B/A::KANSL1 fusion. The mutation landscape varies within the group of sarcomas with the KAT6B/A::KANSL1 fusion, as does the mRNA expression within this group (PCA analysis) and both might be linked to differences in clinical behavior. Our results, together with the results of previously published work, suggest that both the presence of additional molecular alterations (copy number variations or mutations) or the differences in methylation profiling may be used as a surrogate marker in the identification of tumors with aggressive behavior.
Transcriptome analysis comparing the expression profile of sarcoma with KAT6B/A::KANSL1 fusion versus LG-ESS tumors revealed an upregulation of genes primarily involved in DNA replication, cell cycle regulation, and chromatin modification, and a downregulation of several proteasome subunits in the KAT6B/A::KANSL1 group. These differences further support the notion that sarcomas harboring KAT6B/A::KANSL1 fusions are in fact a distinct entity from LG-ESS, as was also suggested in the recent study based on methylation profiles [10]. However, further research is needed to clarify the underlying mechanisms driving these differences.
We are aware of the limitations of our study, which are mainly related to the small number of cases, which makes the comparison between cases with benign and aggressive behavior difficult and impacts the statistical significance of our findings.
In conclusion, the results of our study and previous research suggest that, despite some overlapping morphological and immunohistochemical features with tumors of smooth muscle and endometrial stromal differentiation (LG-ESS and ESN), sarcomas with the KAT6B/A::KANSL1 fusion represent a distinct entity rather than merely a subtype of LG-ESS. It is important to be aware of this entity since despite the commonly bland morphology, the tumors have a propensity for aggressive behavior. Given the sharp circumscription of some tumors, misdiagnosing them as benign lesions, such as endometrial stromal nodule or leiomyoma, can be particularly problematic. Our results suggest that the molecular profile of tumors with aggressive behavior is different from those with benign clinical course, including additional mutations in aggressive cases and differences in mRNA expression. However, further investigation on a larger cohort of cases is needed to confirm these findings.

Comments (0)