
Remember me

The mechanism of the development of MASLD after PD is different from that of conventional MASLD. MASLD usually develops 4–12 months after surgery and may be due to three reasons [4]. First, the impaired pancreatic exocrine function is thought to be the main cause of MASLD after PD [5]. It has been reported that 56.3% of patients who undergo pancreatic surgery develop postoperative pancreatic exocrine insufficiency [8]. Obstructive pancreatitis and pancreatic atrophy occur due to pancreatic duct obstruction by tumors, resulting in decreased exocrine pancreatic function. As a result, impaired fat absorption leads to enhanced conversion of carbohydrates to fat in the liver [5]. Second, the endotoxins induce hepatic dysfunction due to diarrhea and gut barrier dysfunction with zinc deficiency [4, 5]. Intestinal mucosal atrophy is caused by diarrhea due to superior mesenteric artery plexus dissection and impaired pancreatic exocrine function, and bacterial translocation is induced [9]. Furthermore, zinc deficiency also induces diarrhea. Zinc binds to proteins contained in pancreatic enzymes and is absorbed in the duodenum and proximal jejunum, so zinc deficiency is common after PD [10]. As a result, endotoxins inflow into the liver via the PV, activating Kupffer cells and causing fatty deposition in the liver [11]. Third, postoperative malnutrition is suggested to be involved in the development of MASLD after PD [12]. PD is recognized as one of the most challenging operations because of the magnitude of the dissection and resection, and the resultant global stress. Malnourished patients or those who experience major complications after surgery may exhaust their nutritional reserves rapidly and thereby compromise their functional recovery and healing [13]. The decrease in the serum concentration of apolipoprotein B (a major component of very-low-density lipoprotein) caused by a diet deficient in choline induces the impaired hepatic export of triglycerides in the form of very-low-density lipoprotein [14]. As a result, there is a decrease in the export of fat to the outside of the liver, resulting in fatty deposition in the liver.
In our case, SLD was rapidly progressed 2 months after surgery. There were no findings suggesting SLD on CT images obtained on postoperative day 12 or based on liver function tests performed after surgery (Table 1). Although a liver biopsy was not performed because of the risk of bleeding, CT imaging indicated the rapid deterioration of SLD. It has been suggested that an attenuation of 40 Hounsfield units on pre-contrast CT scans might be a practical cutoff value for predicting a liver fat content of 30% [15, 16]. Moreover, a liver-to-spleen ratio of less than 0.9 is considered an indicator of SLD [17, 18]. The SLD in the present case could have been caused by any of the reasons mentioned above. First, regarding nutritional disorders after surgery, the patient’s BMI was 27.3 kg/m2, which is considered obese in Japan and did not decrease after discharge, although she lost approximately 6% of her preoperative weight. Nutritional assessment using the Onodera–Prognostic Nutritional Index [19] showed a tendency toward recovery (Fig. 3). While her lymphocyte count was decreased and she had low levels of albumin and cholinesterase activity, these data appeared to have been within the scope of surgical invasion of PD because the patient was able to maintain her daily life activities. Considering past reports, it is unlikely that the SLD would rapidly worsen while the patient was in this nutritional state [12]. Second, the patient had pancreatitis before surgery and may have developed exocrine pancreatic insufficiency after surgery. The patient was taking pancrelipase for postoperative steatorrhea and this had improved by the time of discharge. In the days before her readmission, the patient had more than 10 bouts of diarrhea. At the time of readmission, the serum zinc concentration had decreased to 40 µg/dl. Considering the patient had pancreatic insufficiency, we initially considered increasing the doses of pancreatic enzymes and zinc supplements; however, we did not do so because if the coagulation function deteriorated further, transhepatic intervention would no longer be possible. Therefore, it was decided to prioritize treatment of the PV. As a result, the portal blood flow improved and the diarrhea symptoms were alleviated. After intervention, the pre-contrast CT values in the liver and the liver-to-spleen ratio returned to preoperative levels (Fig. 4). Considering that the stool quality had been stable and diabetes had not been an issue after intervention, it seems likely that exocrine pancreatic insufficiency was not the direct cause of the diarrhea. The profuse diarrhea might have been caused by small intestinal congestion due to PV stenosis, and it is thought that the SLD rapidly progressed due to impaired intestinal absorption and gut barrier dysfunction associated with zinc deficiency. After the PV intervention, the intestinal edema and L/S ratio on CT were soon improved (Figs. 2d and 4), and there has been no recurrence. The diarrhea symptoms and nutritional markers also gradually improved (Fig. 3). Although zinc levels did not be measured, there were no symptoms of hypozincemia, such as taste disorders. Then, it is considered that the SLD was alleviated by improvement of portal vein flow and absorption in the small intestine.
Fig. 3
Time course of changes in diarrhea symptoms and nutritional markers. The frequency and nature of the stools and the changes in the onodera–prognostic nutritional index (O-PNI) are shown. The O-PNI temporarily worsened after PV intervention, but gradually recovered. The symptoms of diarrhea also gradually improved after intervention
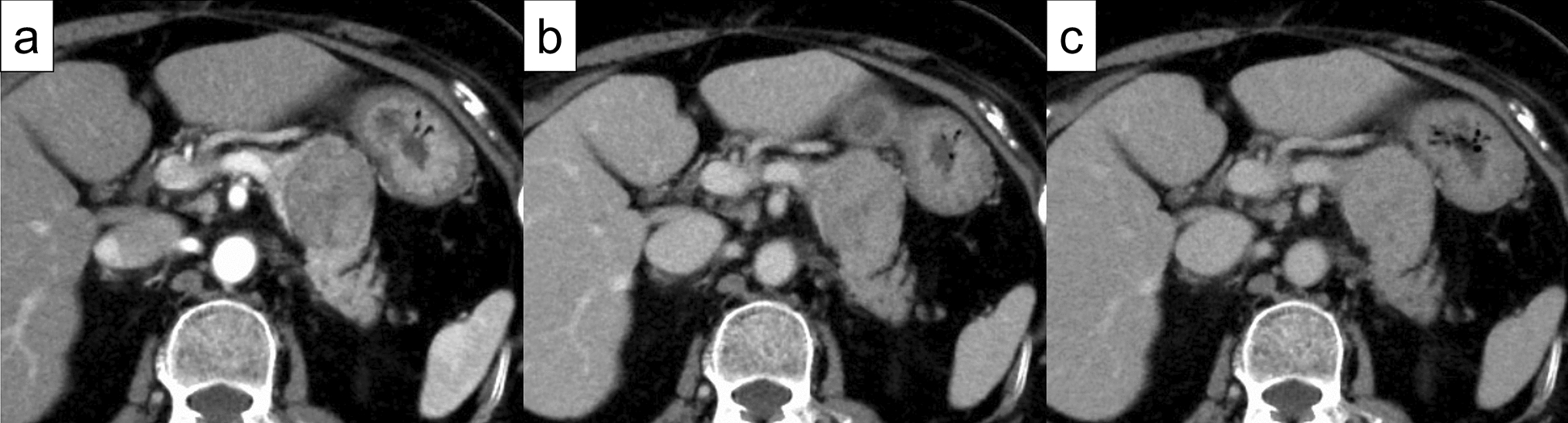
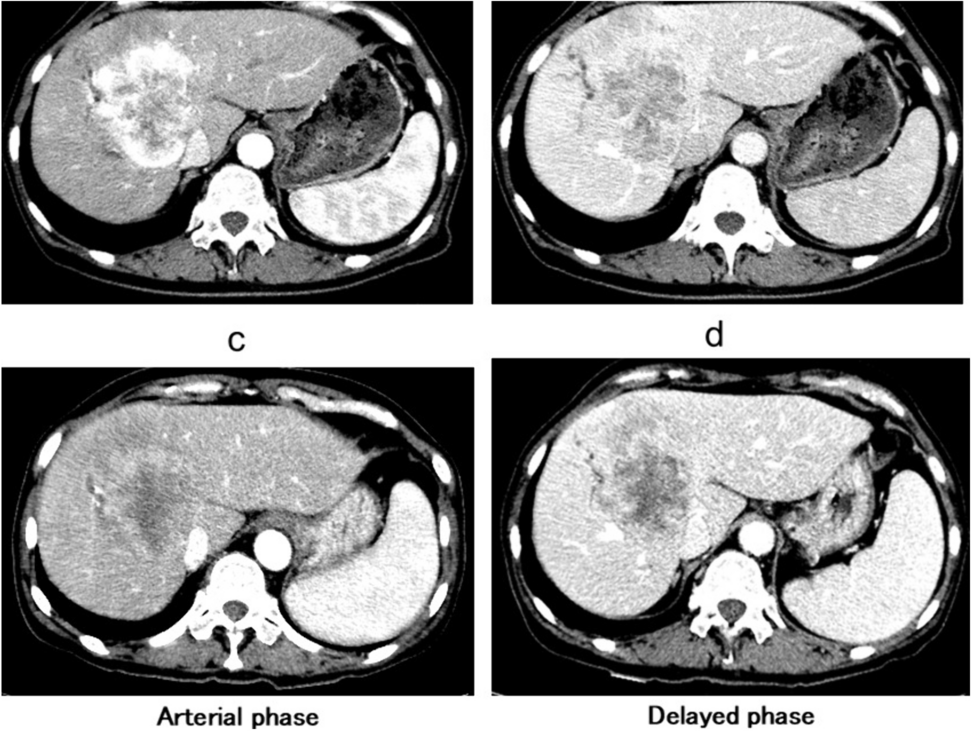
Fig. 4
Changes in the CT images of the steatotic liver over time. a Axial and coronal views of the pre-contrast CT images over time show that the average CT values of the areas at S3, 5, and 8 are decreased due to the PV stenosis. b Average Hounsfield unit values of ten randomly selected parts of the liver and spleen show the gradual improvement in the liver-to-spleen (L/S) ratio after the intervention
PV stenosis has a reported incidence of less than 20% after hepatobiliary surgery that involves resection of the PV and often occurs at 6 months after surgery [20]. The most common cause of PV stenosis is local tumor recurrence, especially pancreatic cancer, while benign stenosis is caused by inflammation of a pancreatic fistula [21, 22]. The early symptoms of PV stenosis are nausea, abnormal liver function test results, intestinal angina-like pain, and ascites, which are signs of portal hypertension [23]. As the pancreatic head, bile duct, and hepatoduodenal ligament are resected and it is difficult to form collateral veins to the liver, gastrointestinal bleeding is likely to occur [20]. In our case, the PV stenosis was thought to be caused by inflammation, as the preoperative pancreatitis was severe and a drain infection occurred after surgery. Ultrasonography confirmed that the flow of the intrahepatic PV was maintained; however, early treatment was deemed necessary because the disease was progressive. PV stenting is a safe and effective treatment for postoperative PV stenosis [24, 25].
In conclusion, we experienced a case of MASLD after PD in which the patient’s condition rapidly deteriorated with diarrhea and impaired intestinal absorption due to PV stenosis. MASLD after PD might develop for various reasons, so it is necessary to carefully monitor the postoperative recovery.
Comments (0)