
Remember me

A 71-year-old man received interferon therapy for hepatitis C in 2009. Despite the sustained virological response to hepatitis C, HCC developed in S2 and S3 in December 2016, and lateral segmentectomy was performed. In October 2017, lymph node metastases were identified near the hepatic hilum, hepatoduodenal ligament, and peritoneal dissemination node and recurrence were diagnosed. In November 2017, disseminated lesion resection and cholecystectomy were performed, and the patient was referred to another hospital for subsequent treatment. In December 2017, contrast-enhanced computed tomography (CT) revealed that there were still many peritoneal nodules. Sorafenib was started in January 2018, followed by lenvatinib, regorafenib, and ramucirumab. However, the patient did not respond to the treatment, and liver metastasis and peritoneal dissemination were aggravated in August 2020. The patient visited our hospital for further treatment of HCC in September 2020.
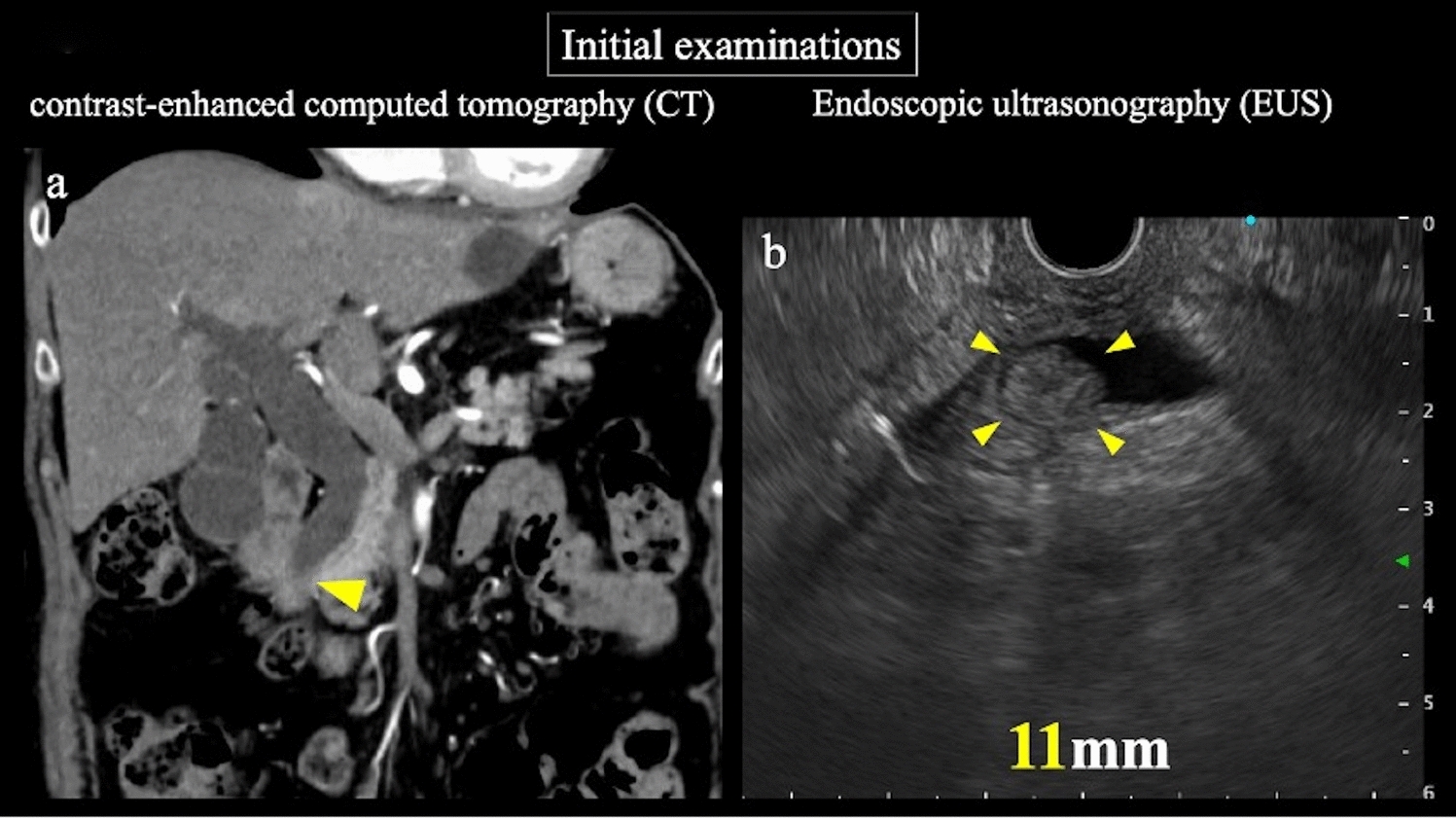
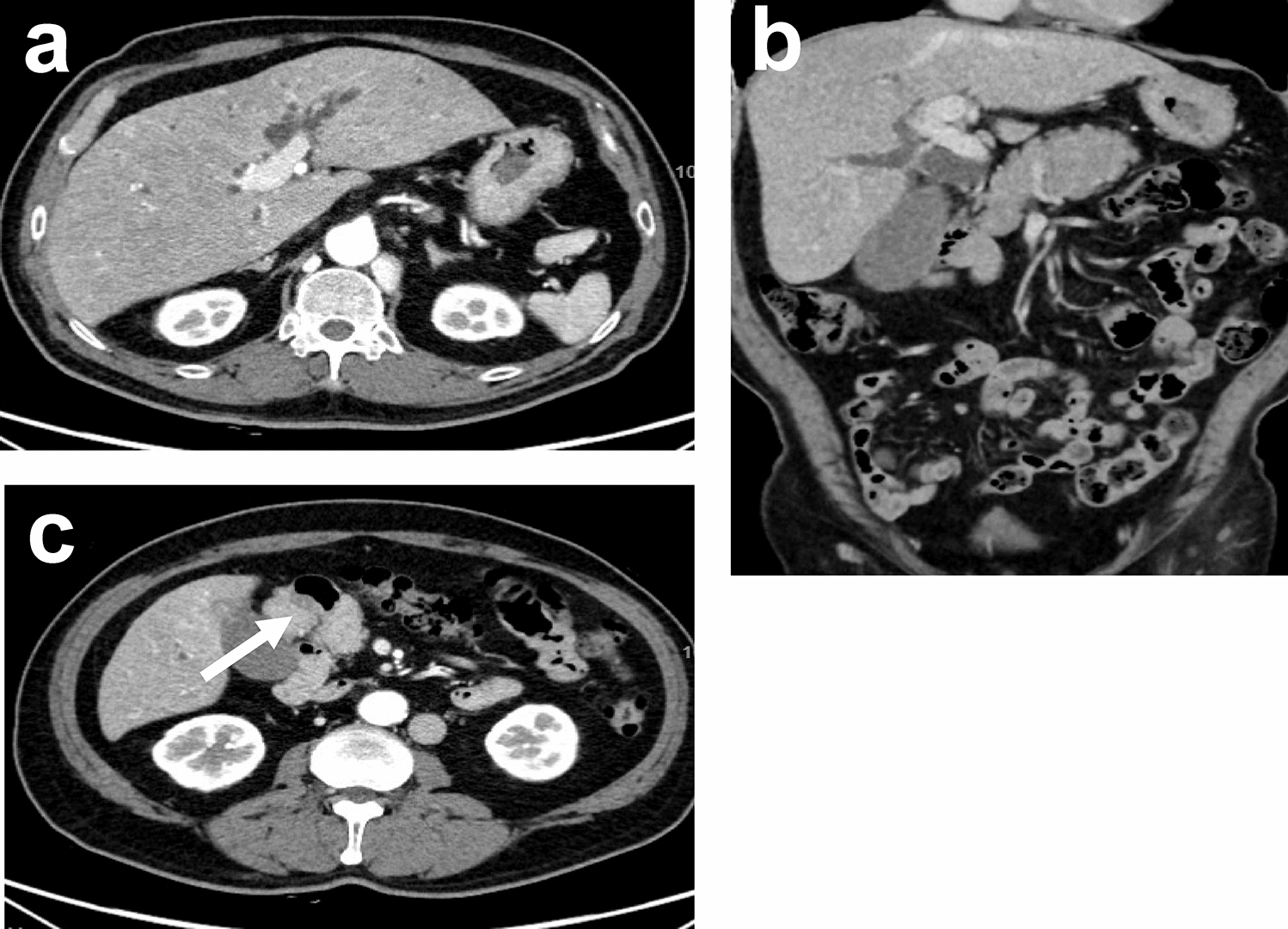
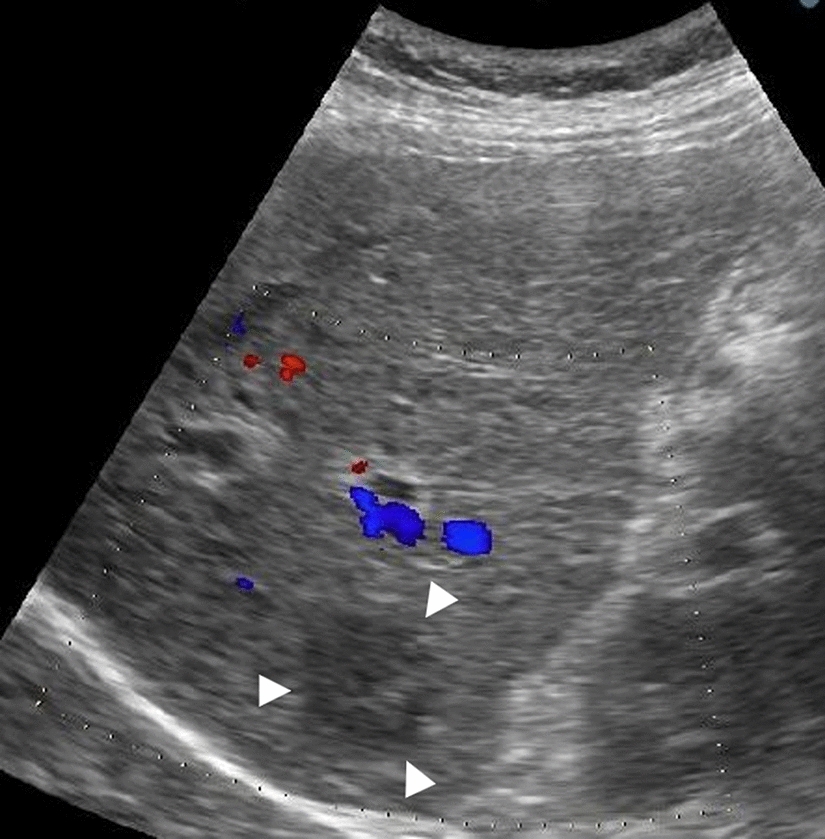
Contrast-enhanced CT revealed an HCC with a maximum diameter of 10 cm centered on hepatic segments 5 and 8, with a peritoneal dissemination nodule measuring 22 mm in maximum diameter near the hepatoduodenal ligament and a maximum diameter of 35 mm near the omentum (Fig. 1). Minimal ascites was observed on the liver surface, raising suspicion of peritoneal dissemination. On admission, the patient was Child–Pugh class A, with a score of 5. First, we performed transcatheter arterial chemoembolization (TACE) on the intrahepatic lesions to control the tumor and prevent bleeding owing to tumor rupture. Post-treatment CT showed attenuation of enhancement in the intrahepatic lesions; however, intrahepatic lesions and peritoneal dissemination progressed (Fig. 2a). Therefore, we initiated atezolizumab and bevacizumab therapy on November, 2020. There were no obvious treatment-related adverse events; however, progression of all lesions was observed on contrast-enhanced CT after the administration of the second course of atezolizumab and bevacizumab on December, 2020 (Fig. 2b). Alpha-fetoprotein (AFP) and des-gamma-carboxyprothrombin (DCP) levels temporarily decreased but increased again after two courses of administration. Based on these findings, we diagnosed the patient with progressive disease (PD) and terminated atezolizumab and bevacizumab therapy. Subsequently, cabozantinib treatment (60 mg orally once daily) was initiated on January, 2021. Although liver enzymes were not elevated before the initiation of cabozantinib therapy, grade 3 increases in aspartate aminotransferase and alanine aminotransferase levels (386 IU/L and 105 IU/L, respectively) and anorexia, and grade 1 nausea and vomiting (according to the Common Terminology Criteria for Adverse Events [CTCAE] version 5.0) were observed 1 week after the start of cabozantinib treatment (Table 1). Contrast-enhanced CT showed attenuation of enhancement in the liver lesion and peritoneal dissemination (Fig. 2c), and tumor markers (including AFP and DCP) decreased (Fig. 3, Table 2). However, the decrease in performance status was significant even after treatment interruption, and patients with grade 3 anorexia did not recover. Therefore, we thought that these symptoms resulted from disease progression, and he received only the best supportive care thereafter. His physical condition and activities of daily living had worsened, making it difficult for him to visit the hospital. Finally, the patient and his family opted for home care.
Fig. 1
Contrast-enhanced computed tomography upon admission to our hospital
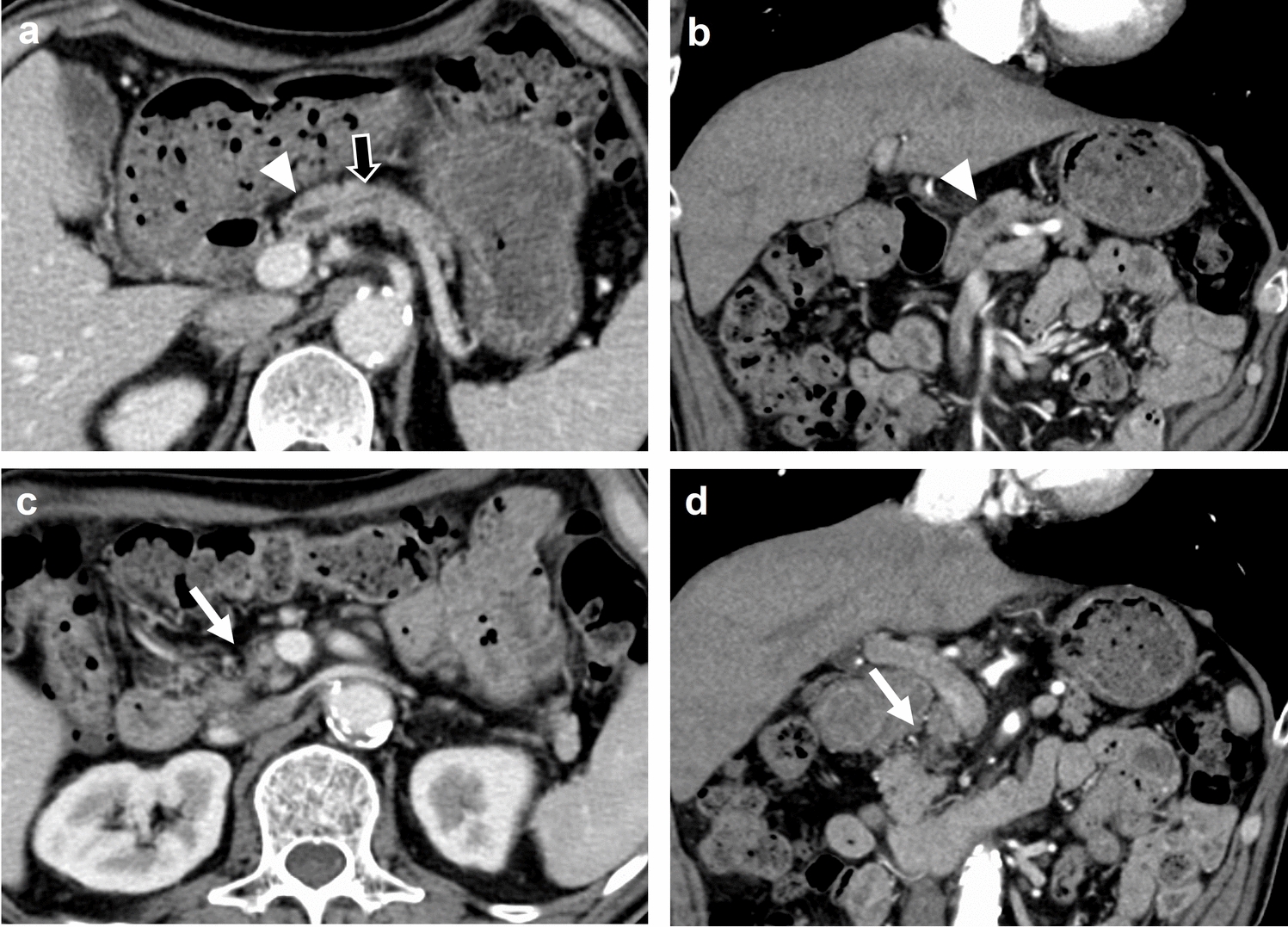
Fig. 2
Changes in contrast-enhanced computed tomography image after treatment in our hospital
Table 1 Laboratory findings after cabozantinib administrationFig. 3
Tumor markers upon admission to our hospital
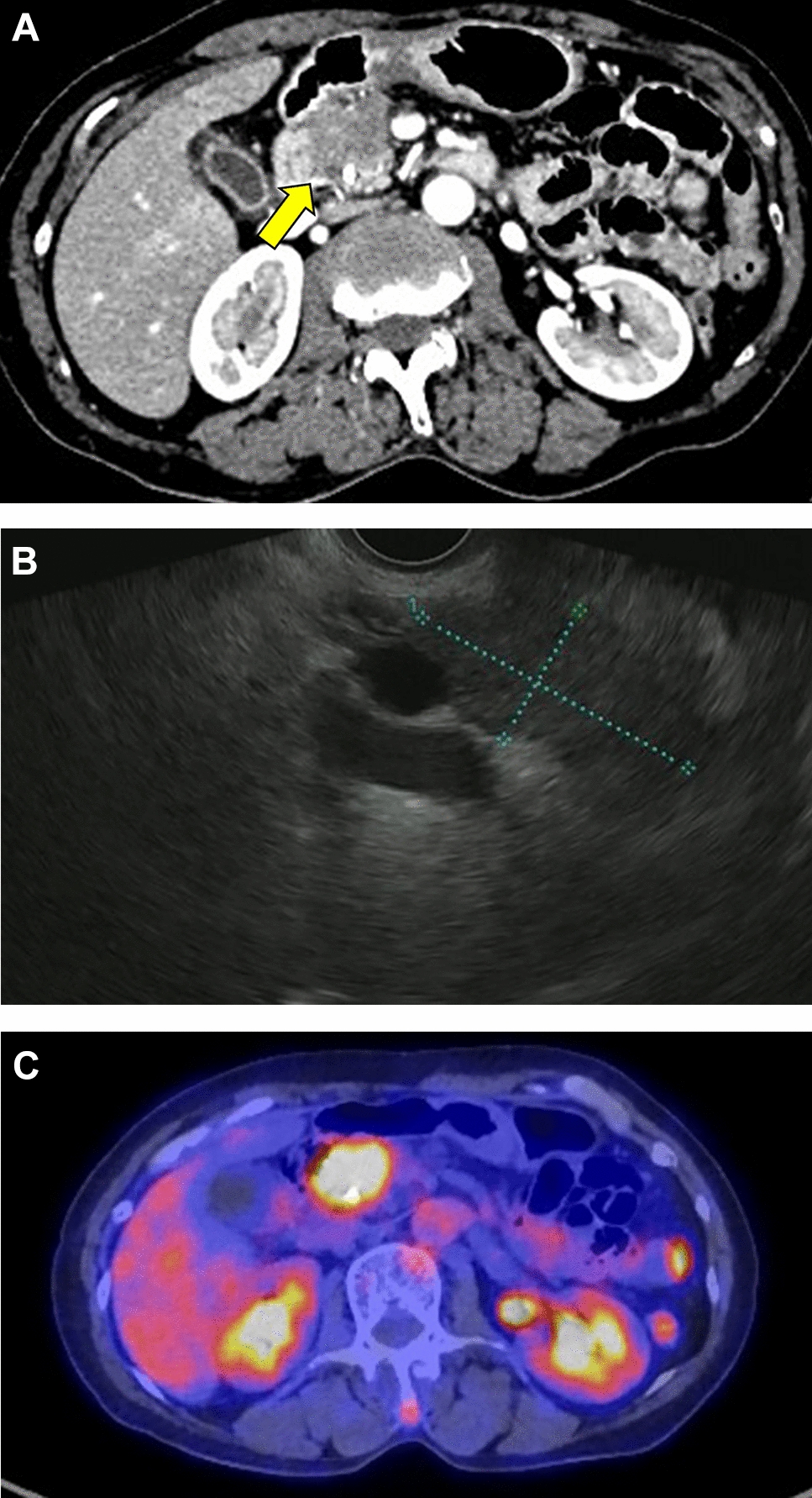
Table 2 Tumor markers from admission to follow-up after treatmentAlong with continued supportive care at home, the symptoms of anorexia and oral intake gradually improved, as did his physical condition. He visited our hospital in June 2021. Contrast-enhanced CT showed attenuation of blood flow in the intrahepatic lesion and peritoneal dissemination nodules, and the tumor size decreased, leading to a diagnosis of CR according to mRECIST (Fig. 2d). The tumors did not progress until April 2022 without any treatment for HCC; however, partial recurrence with increased blood flow on contrast-enhanced CT was observed under the hepatic capsule, leading to a diagnosis of hepatic local recurrence. As there was no obvious recurrence, except for this lesion, carbon-iron radiotherapy (60 GyE/12 fractions) was initiated from June 2022. He has been free from tumor progression and was reported alive until November 2023 (34 months after CR).
Comments (0)