FGP is a benign gastric polyp, often found in the stomach without atrophic changes, and occurs both syndromically and sporadically, with background disease in the former, including FAP and GAPPS [3, 4]. Sporadic FGP is known to be associated with PPI use, and its frequency has increased with the recent increase in PPI use [5, 6]. Its frequency varies among reports; however, in the general population, it ranges from 1.8% to 5.9%, with a predilection for middle-aged women [1, 7]. Syndromic FGP is often associated with epithelial dysplasia; however, sporadic FGP with high-grade dysplasia or adenocarcinoma is extremely rare [8]. Recent studies have suggested that long-term gastric acid suppression is associated with carcinogenesis, but these studies have been limited to gastric cancer after HP eradication [9, 10]. It is unclear whether HP-uninfected gastric cancers are associated with long-term gastric acid suppression, perhaps because HP-uninfected gastric cancers are a small proportion of all gastric cancers. Sporadic FGPs show a high probability of activating mutations in CTNNB1 (encoding β-catenin) [11], while syndromic FGPs are caused by inherited germline mutations in the adenomatous polyposis coli (APC) gene with somatic second hit mutations [12]. Non-dysplastic sporadic FGPs only have activating mutations in CTNNB1, whereas dysplastic FGPs, both sporadic and syndromic, have been reported to have truncating mutations in the APC gene [13]. In the present case, the absence of colorectal cancer in the patient's family history and the absence of adenomatous polyposis on colonoscopy suggested that the lesion was a gastric adenocarcinoma occurring in sporadic FGP that had increased with oral PPIs. However, our institution was not equipped to carry out genetic analysis, and we could not perform it.
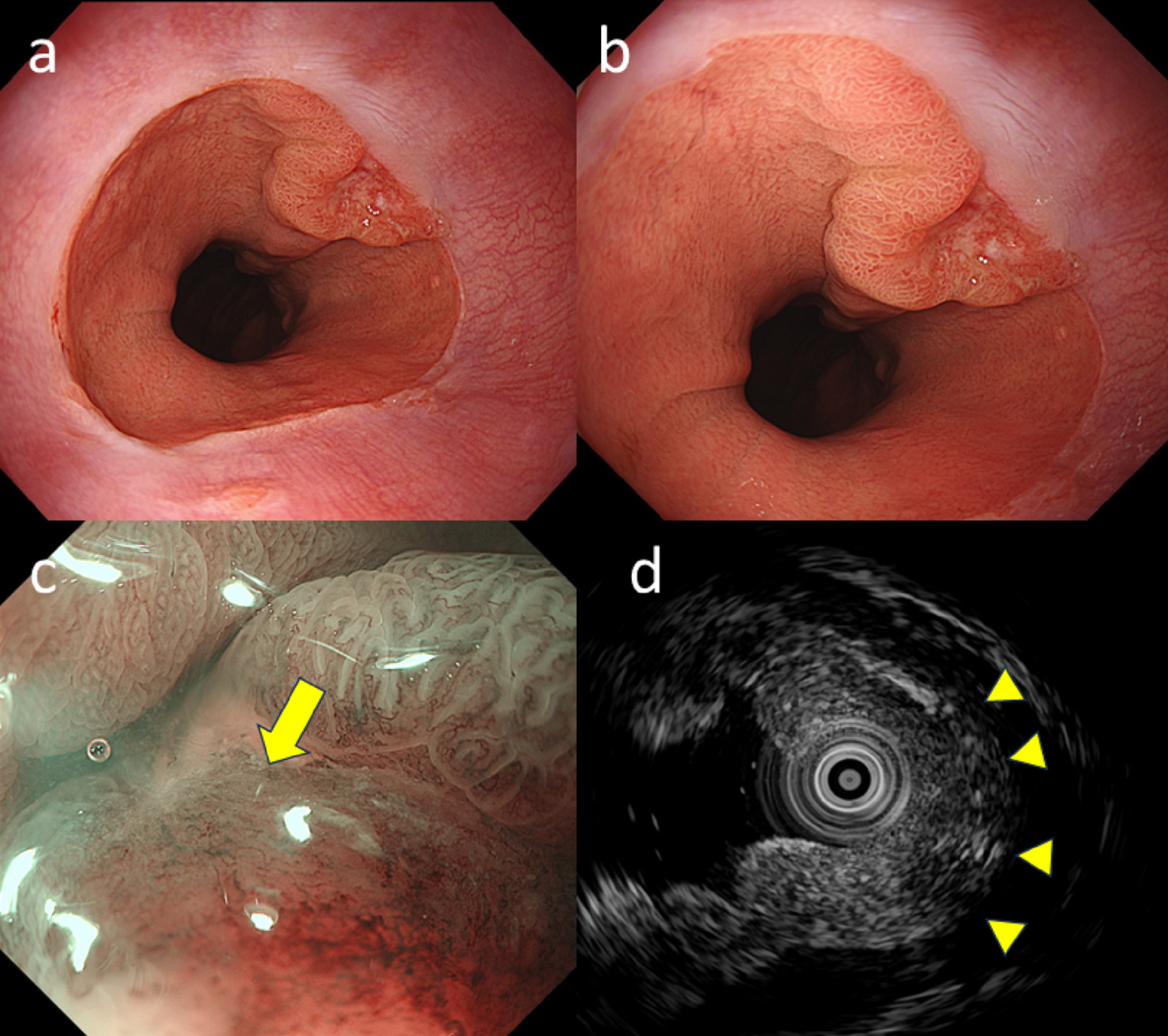
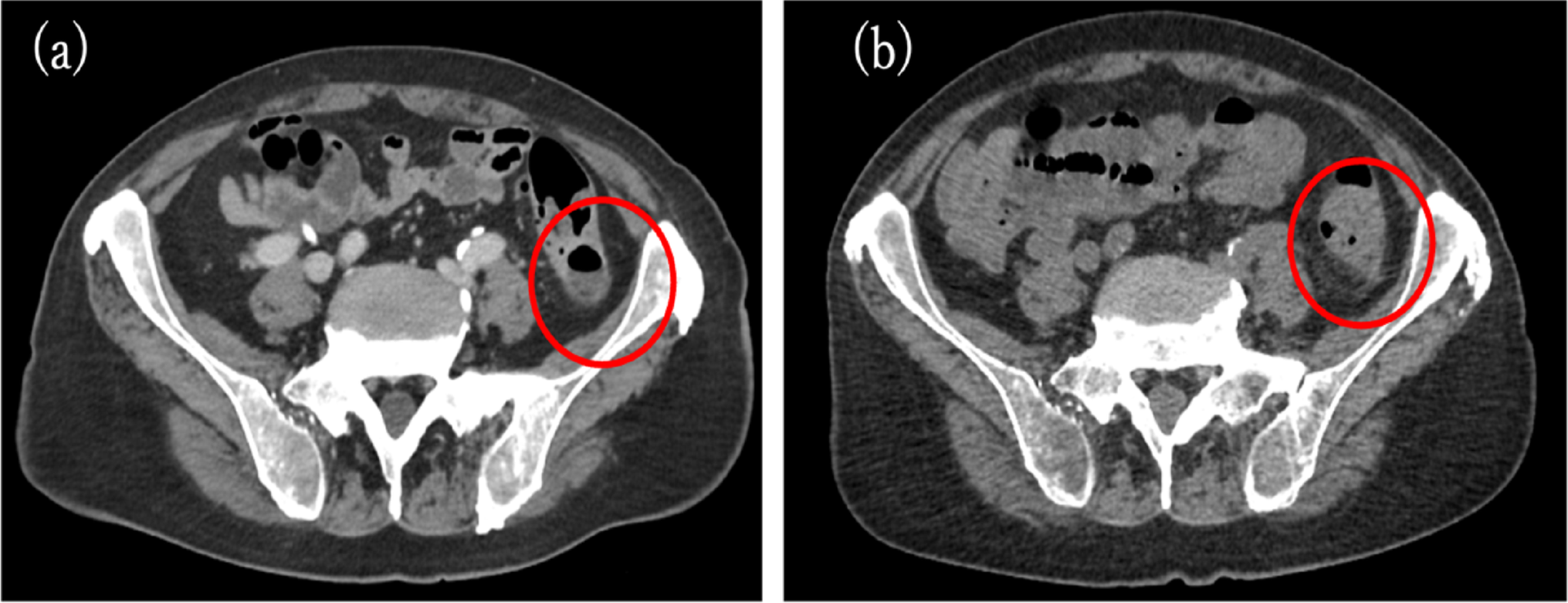
To the best of our knowledge, only six cases of sporadic FGP with high-grade dysplasia or adenocarcinoma have been reported, and none of them were invasive carcinomas [14,15,16,17,18]; five of the six cases were without HP infection, and the remaining one occurred after HP eradication. Two of the five cases in which PPI use was mentioned were on PPIs for long periods (5 and 14 years). Of the six cases, four had a reddish tone. The remaining two cases did not mention the color tone. In this case, there was no evidence of HP infection, the patient had been on PPI for 6 years, and the lesion was observed to be reddish; although FGP is essentially isochromatic, the reddish color of FGP suggested the possibility of adenocarcinoma. Furthermore, FGP enlarged by PPI regresses in approximately 2 months [19]. In this case, the lesion also reduced in size from 25 to 15 mm after discontinuation of PPI for 1 month. Therefore, even if the PPI withdrawal resulted in a reduction of the lesion, malignancy cannot be ruled out. Furthermore, in pathological findings, foveolar cell proliferation and parietal cell protrusion, which are typical findings in PPI-associated FGPs [20, 21], were not prominent, suggesting the possibility of regression due to PPI withdrawal.
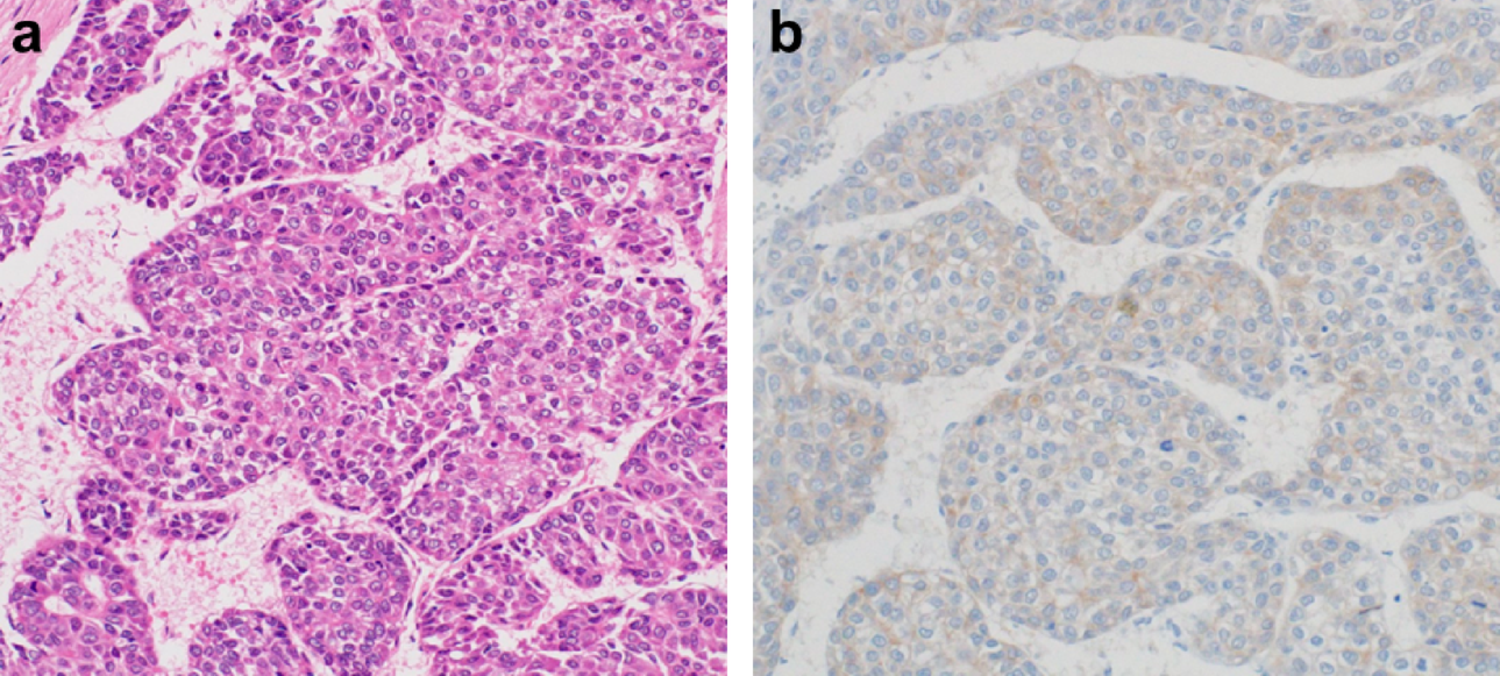
In immunochemical staining, Jalving et al. [22] and Nawata et al. [18] reported that nuclear staining for β-catenin was observed in sporadic FGP dysplasia and that activation of the Wnt–APC-β-catenin pathway may be involved in the development of dysplasia, but in this case, no nuclear staining for β-catenin was observed. There are also reports that no nuclear staining for β-catenin was observed in sporadic FGP dysplasia, suggesting that pathways other than the APC-β-catenin may be involved in the development of FGP high-grade dysplasia or adenocarcinoma [14, 16, 17]. The overexpression of p53, which is not typical of FGP dysplasia [23], was observed in this case. The patient had a history of ulcerative proctitis, which is known to be associated with p53 mutations at an early stage in ulcerative colitis-related neoplasms [24]. However, there are no reports of gastric cancer complications being more common in patients with ulcerative colitis or of p53 mutations being more likely to occur in the gastric mucosa, and no association has been demonstrated [25]. Furthermore, this case showed that MUC5AC and MUC6 were positive, and MUC2 was partially positive in the cancerous area, indicating the development of a gastrointestinal phenotype. Although the expression of the gastric phenotype has been reported in high-grade dysplasia or adenocarcinoma occurring with sporadic FGP in HP-uninfected patients [16,17,18], the expression of the gastrointestinal phenotypes has been reported at a certain frequency in HP-uninfected gastric cancers [26, 27]. The gastrointestinal types are considered to be derived from various cell types and are presumed to be the result of multifactorial carcinogenesis. Based on these results, the possibility of multifactorial carcinogenesis was also suspected in gastric cancers occurring in sporadic FGP.
Gastric adenocarcinoma of fundic-gland type (GA-FG) has been reported to be the most common type of HP-uninfected gastric cancer [28]. GA-FGs occur in the upper part of the stomach and are identified by endoscopic findings as having an elevated shape, especially a submucosal tumor (SMT)-like shape, or a flat or depressed shape [29]. GA-FGs are known to infiltrate the submucosa more frequently among HP-uninfected gastric neoplasms. GA-FGs are immunohistochemically positive for pepsinogen-I, H + /K + ATPase and MUC6 staining. A subtype of GA-FG, gastric adenocarcinoma of fundic-gland mucosa type (GA-FGM), has also been proposed, which differs from GA-FG by being positive for MUC5AC [29]. In the present case, MUC5AC and MUC6 were positive, but pepsinogen I and H + /K + ATPase were negative, showing a different immunostaining attitude and not meeting the definition of GA-FGM. Furthermore, the endoscopic findings were not the SMT-like shape characteristic of GA-FGM, but a well-defined borderline elevated lesion.
In summary, we experienced a case of gastric invasive adenocarcinoma occurring in sporadic FGP without an HP infection. The unusual endoscopic findings of rapid enlargement and reddish tone pushed us to perform endoscopic treatment, which resulted in a correct diagnosis and appropriate treatment.

Comments (0)