
Remember me
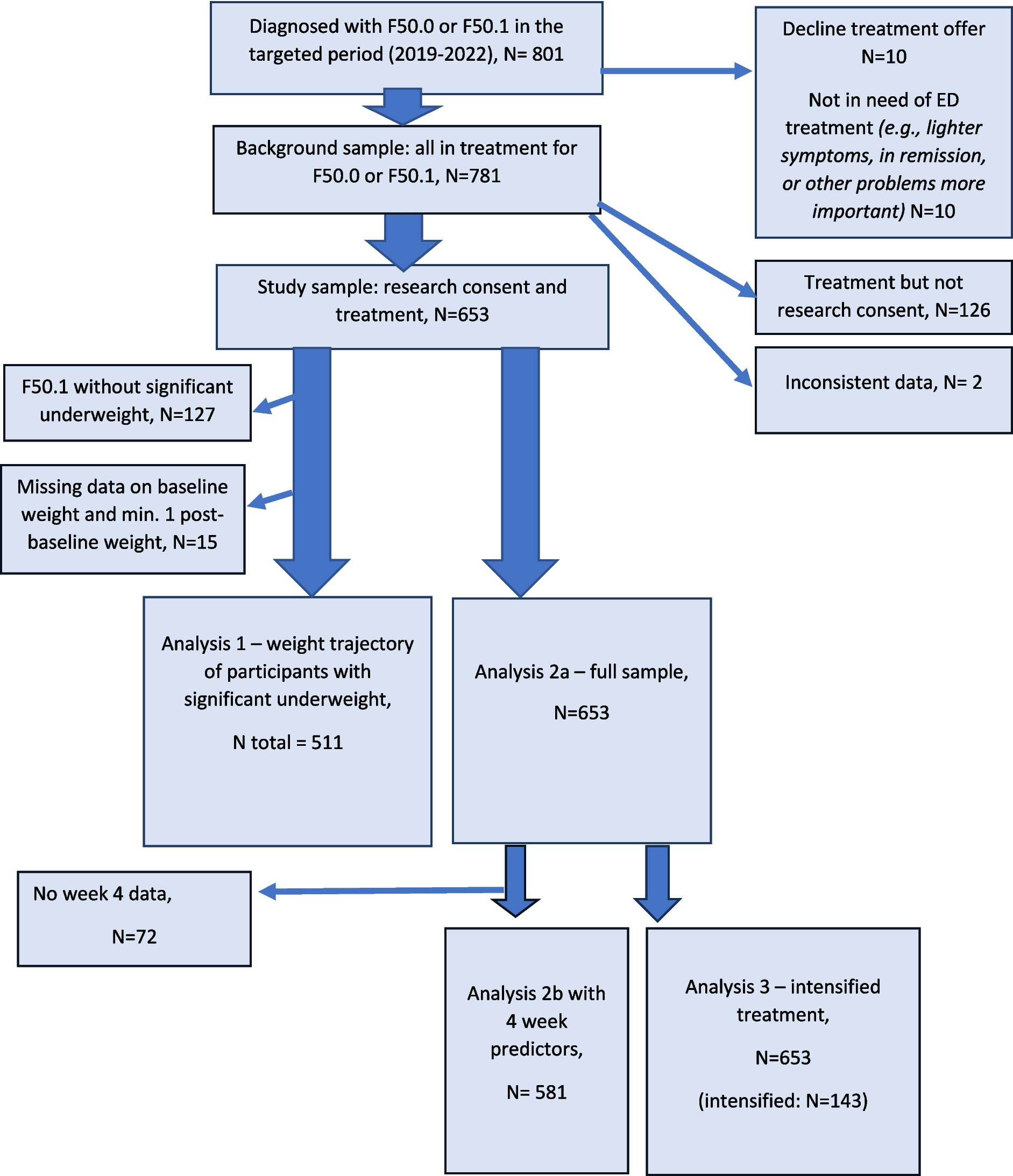
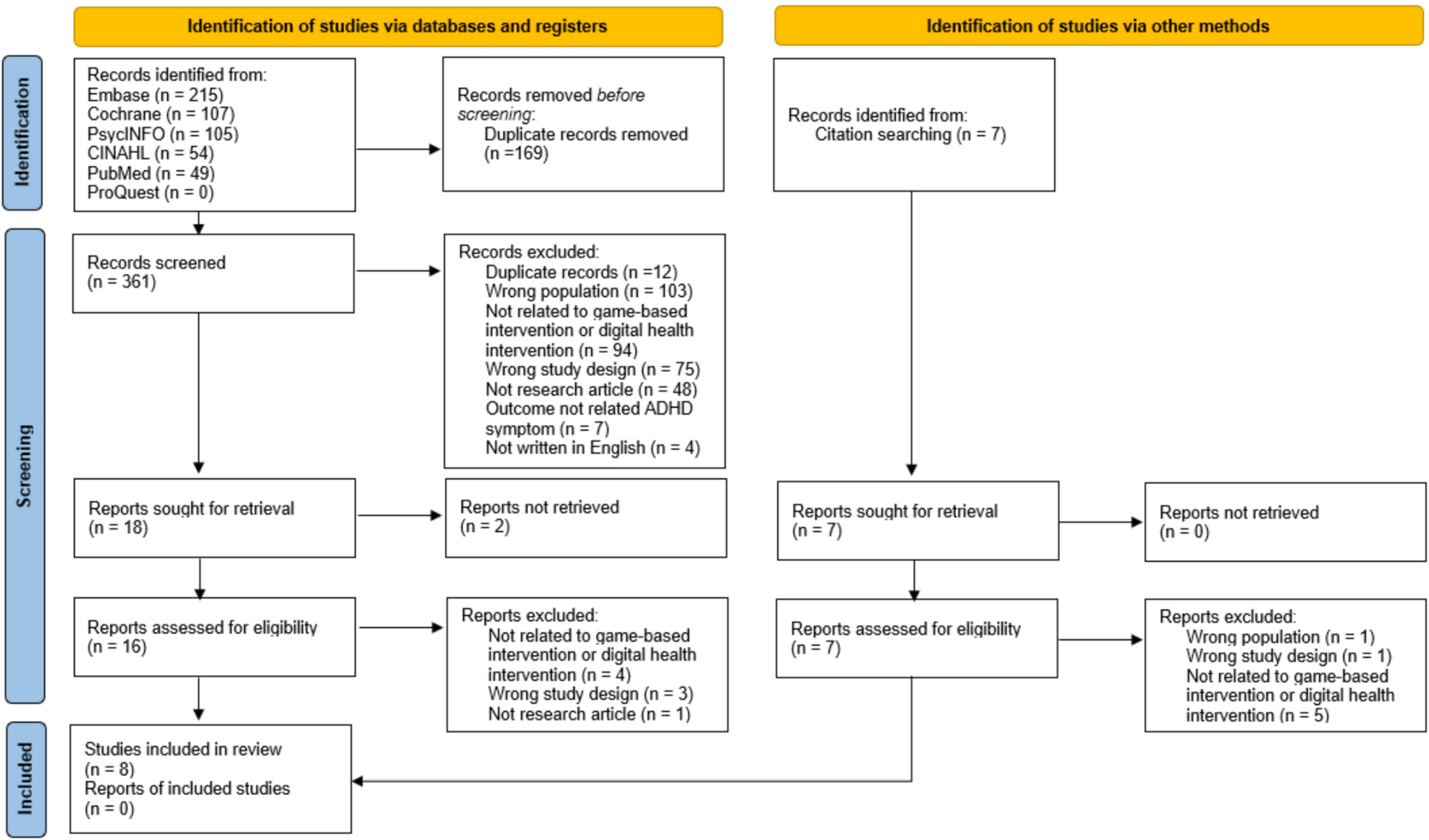
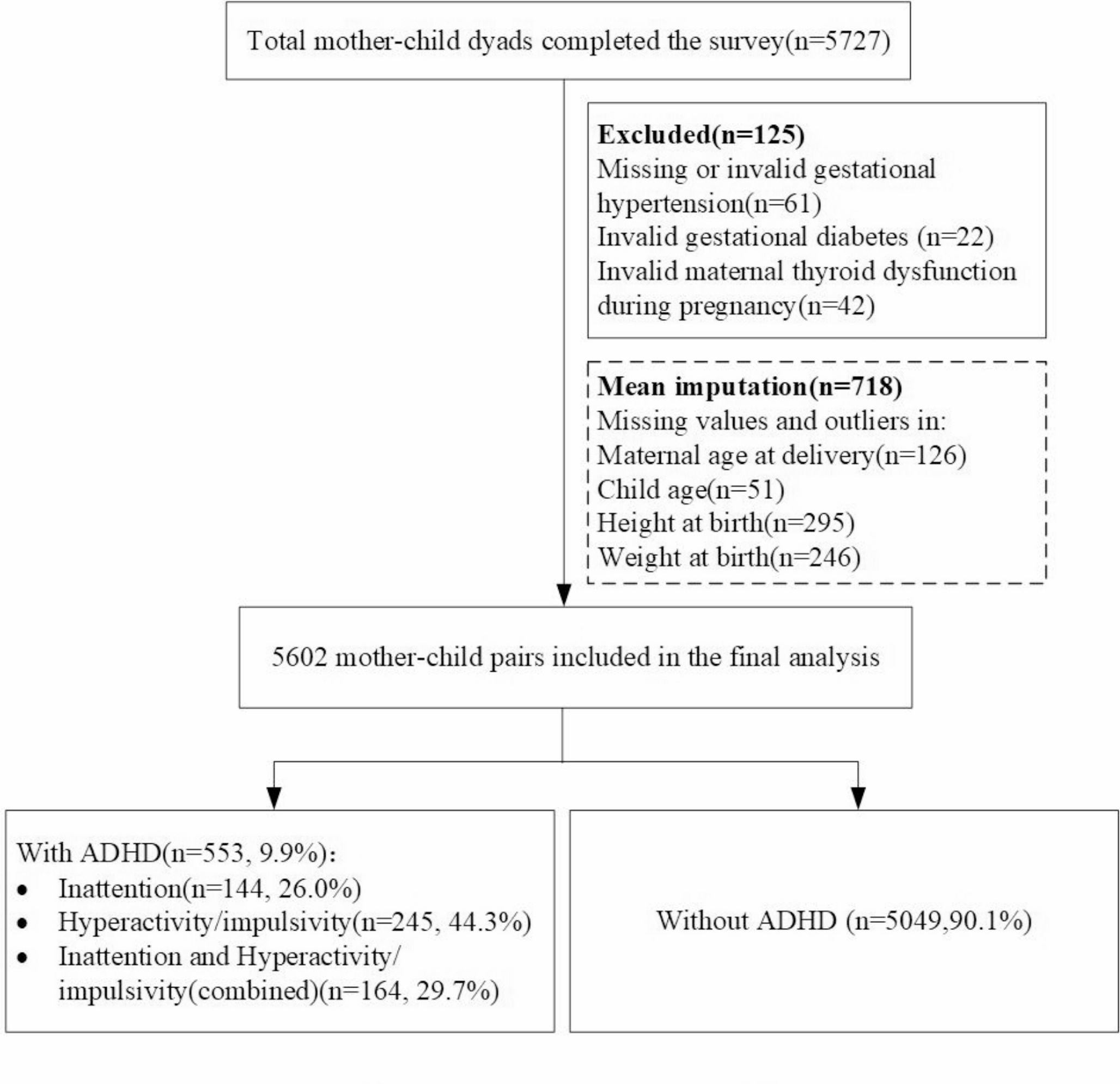
Out of 4088 studies, 69 studies were included in the review (Fig. 1), with 31 quantitative, 23 qualitative, and 15 mixed-methods studies.
Study characteristics are described in Online Resource 2. Fifty-nine studies (86%) were conducted in high-income countries, including Australia and New Zealand (n = 20, 29%), the US and Canada (n = 14, 20%), UK (n = 8, 12%), and Sweden (n = 5, 7%). Sample sizes varied widely: ranging from 4 to 118 in qualitative and from 14 to 7849 in quantitative components. Barriers/facilitators in using W-MHIs were reported from YP (n = 63, 91%), healthcare providers (n = 17, 25%), and parents (n = 8, 12%). Of 63 studies reporting YP’s perspectives, 27 studies (46%) targeted adolescents under 19 years, 21 (36%) targeted YP aged between 16 and 25 years, and the remaining targeted cohorts aged 10–25 years. Four studies targeted minority groups, including black young men [42], LGBTIQA + people [43, 44], and YP of a refugee background [45]. The study population was predominantly young women (n = 54, 86%). Barriers/facilitators were captured either qualitatively (i.e., interviews (41%), focus groups (13%)), or quantitatively (i.e., self-reported surveys using rating scale (57%) or open-ended questions (9%), or observational methods (3%)).
Intervention characteristicsOf the 69 included studies, 58 studies (84%) reported participants’ feedback of using a specific intervention and the remaining studies explored general W-MHIs without focusing on a specific program. Intervention characteristics are presented in Online Resource 3.
Forty-two studies (61%) reported interventions targeting anxiety, depression, and/or stress, three (4%) targeted obsessive–compulsive disorder, three (4%) targeted suicidal ideation, and two (3%) targeted eating disorders. The remaining (n = 19, 28%) targeted mental wellbeing without a specific condition. The included interventions were primarily delivered via a website only (n = 61, 88%). Other platforms included web-apps (e.g., delivered via a website and an app) (n = 6, 9%), and a combination of web-based and face-to-face sessions (n = 2, 3%). The majority of W-MHIs were based on CBT (n = 37, 54%). Other approaches included psychoeducation (n = 4, 6%), social networking (n = 2, 3%), positive psychology (n = 2, 3%), and a combination of different approaches (n = 10, 14%). The remaining studies did not report the intervention approach.
Overall, 39 studies reported guided W-MHIs, 16 reported unguided W-MHIs, and 14 did not specify. The guidance was provided by health professionals (e.g., therapists, clinicians, and physicians) or non-health professionals (e.g., school staffs), reported in 24 and 13 studies, respectively. Peer support was embedded in four interventions. Intervention duration varied, ranging from single to 40 sessions and each session lasted between 5 and 60 min.
Due to the great variance in study methodology, study population and interventions, a meta-analysis was infeasible.
Barrier/facilitator themesBarriers/facilitators from YP’s, healthcare providers’, and parents’ perspectives are summarized below. Barriers/facilitators identified in each study are provided in Online Resource 4.
Young people’s barriers and facilitators of engagement with W-MHIsThere were 63 studies reporting YP’s perspectives regarding their barriers/facilitators of engagement with W-MHIs. Three overarching themes were developed, including practical factors, intervention-specific factors, and individual-specific factors. There was some overlap among themes due to the influence of factors associated with user’s perception and behavior to use. For instance, user-specific factors (e.g., perceived need and interest) might drive user’s perceived program usefulness. Intervention-specific factors (e.g., program features and usefulness) might impact user interest in W-MHIs, consequently influencing user engagement. Barriers/facilitators were reported more frequently in qualitative studies than quantitative studies, with the exception of sociodemographic variables. A summary of subthemes and their distributions across all studies are outlined in Fig. 2.
Fig. 2
Young people’s barriers and facilitators of engagement (n = 63 studies)
Theme 1: practical factorsConvenience but lack of timeTwenty (32%) studies found that YP’s engagement with W-MHIs was facilitated due to the accessibility that allowed them to access it anywhere and at any time [42, 46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62] and the ease of incorporating their use into YP’s schedule [50, 57, 58, 63]. This facilitator was endorsed by 59–95% of YP [46, 49, 51, 52, 56]. In contrast, some YP preferred to complete sessions on schedule [54]. Lack of time or busyness was a barrier (n = 18, 29%) [45, 46, 48, 51, 53, 54, 56, 57, 62, 64,65,66,67,68,69,70,71,72,73], endorsed by 42–76% of participants [56, 65, 67, 69].
Ease of use and technical factorsBeing easy to use was a facilitator of engagement (n = 23, 37%) [43,44,45,46, 54, 57, 58, 63, 74,75,76,77,78,79,80,81], endorsed by 63–90% of study participants [46, 52, 56, 68, 69, 74, 82,83,84]. Disengagement could be caused by technical factors (n = 20, 32%), primarily related to connection issues [43, 46, 55, 57, 68, 73, 79] and if the program was not working properly [54, 58, 62, 79, 85].
CostLow cost of access was identified as a facilitator in five studies [56, 57, 59, 60, 78]. Despite the relatively low cost compared to in-person therapies, cost of W-MHIs was reported as a barrier in one study [59].
Theme 2: intervention-specific factorsPerceived usefulness or unhelpfulnessPerceived usefulness of W-MHIs was the most frequent intervention-related facilitator of engagement (n = 44, 70%). Perceived unhelpfulness was a barrier to YP’s engagement (n = 18, 29%). Program usefulness was assessed quantitatively in 20 studies. There were mixed views: 27–88% of participants perceived the program as useful [56, 60, 71,
Comments (0)