Anonymized data are publicly available for purchase from JMDC Inc.
Study population
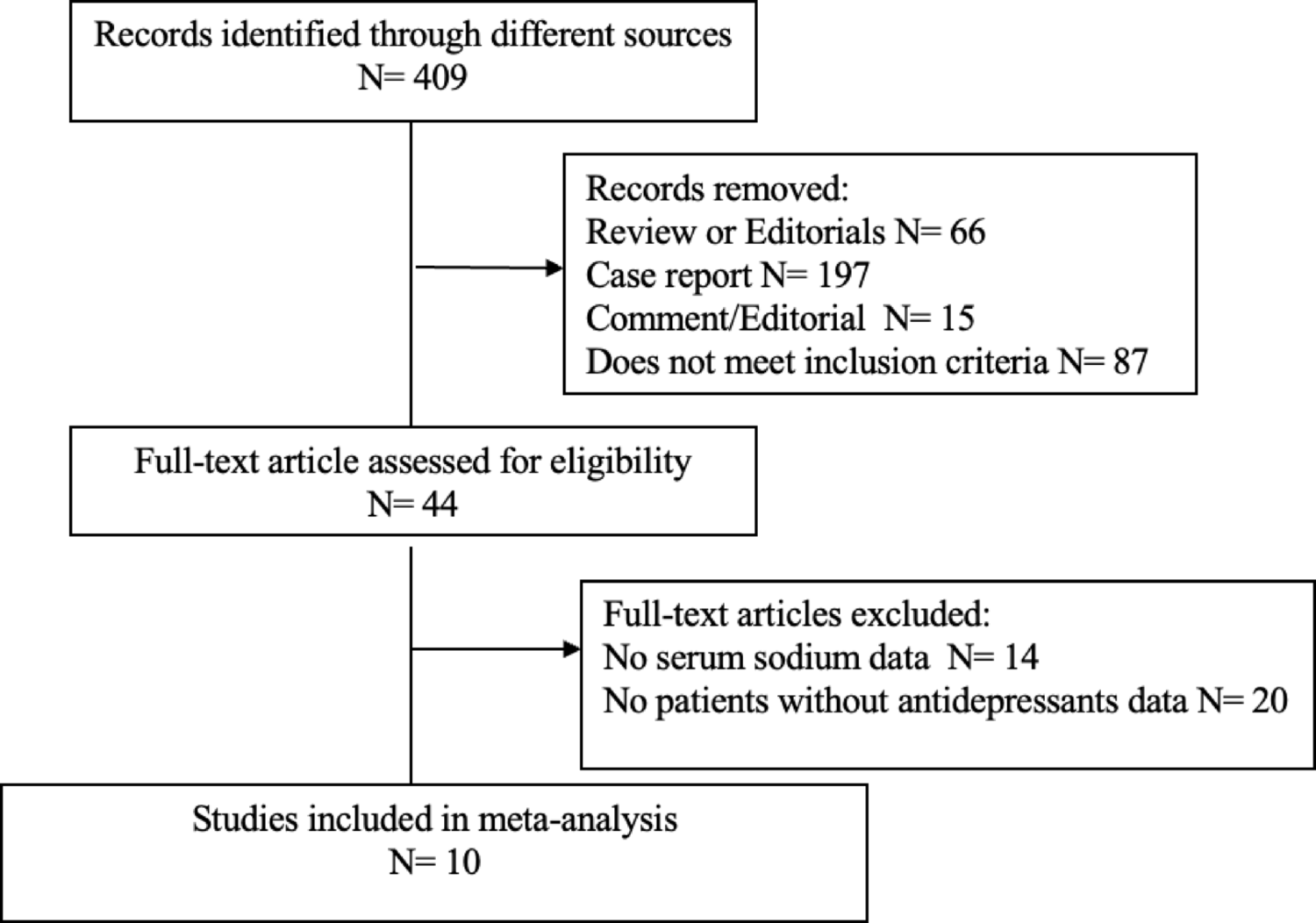
This retrospective cohort study used the JMDC Claims Database, a large-scale administrative claims database [19,20,21]. The JMDC includes annual health checkup data (e.g., blood tests and anthropometric measurements) and health insurance records between 2005 and 2022. In Japan, annual health checkups for employees are a legal requirement. The JMDC Claims Database accumulates insurance claims data. Medical diagnoses were coded according to the International Classification of Diseases, 10th revision (ICD-10). We extracted the data of 21,883 individuals with DM (ICD-10 codes E10–E14) and MAFLD defined as ICD-10 codes of E10–E14 and fatty liver index (FLI) ≥ 30 [22, 23], who newly initiated SGLT2 (empagliflozin, dapagliflozin, canagliflozin, ipragliflozin, tofogliflozin, and luseogliflozin) or dipeptidyl peptidase 4 (DPP4) inhibitors (Supplementary Fig. 1). FLI was calculated using the following formula: FLI = 1/1 + e−(0.953×ln(triglycerides) + 0.139×(BMI) + 0.718×ln(γ−glutamyl transpeptidase [γ−GTP]) + 0.053×(waist circumference)−15.745) × 100. We defined initiating either drug class among individuals who had not previously used either drug class within the previous year as a new use. Furthermore, only individuals with available repeated data for the assessment of FLI during health checkups were included in this study. Among 21,883 individuals, we excluded participants for the following reasons: age < 20 years (n = 1); a history of liver disease defined as liver cancer (ICD-10 code: C22), fibrosis and cirrhosis of the liver (ICD-10 code: K74), hepatitis B (ICD-10 code: B16), hepatitis C (ICD-10 code: B182), autoimmune hepatitis (ICD-10 code: K754), and cholangitis (ICD-10 code: K830) (n = 317); and missing cigarette smoking (n = 262), alcohol consumption (n = 1257), and physical activity (n = 521) data. Finally, 19,525 individuals were included in this study (Supplementary Fig. 2).
Ethics
This study was approved by the Ethics Committee of the University of Tokyo (approval number: 2018-10862), and informed consent was not required because all data included in the JMDC Claims Database were anonymized and de-identified.
Measurements and definitions
We obtained the following data from the health checkups: body mass index (BMI), waist circumference, blood pressure, laboratory data (fasting plasma glucose, hemoglobin A1c [HbA1c], low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, triglycerides, aspartate aminotransferase [AST], alanine aminotransferase [ALT], and gamma-glutamyl transpeptidase [γ-GTP]), cigarette smoking (current or noncurrent/never), alcohol consumption (daily or not every day), and physical activity (active or inactive). Cigarette smoking and alcohol consumption were assessed using a self-report questionnaire during the health checkup. Physical inactivity was defined as not exercising for 30 min ≥ 2 times a week or not walking for more than an hour per day. Based on the ICD-10 code, we obtained data on the presence of diabetic nephropathy (ICD-10 codes: E102, E112, E122, E132, and E142), diabetic retinopathy (ICD-10 codes E103, E113, E123, E133, and E143), and diabetic neuropathy (ICD-10 codes: E104, E114, E124, E134, and E144) at the prescription date of SGLT2 or DPP4 inhibitors. Data on concomitant medications at the prescription date of SGLT2 or DPP4 inhibitors were extracted from administrative claims records.
Propensity score matching
A propensity score matching algorithm was used to generate a matched cohort to compare the benefits of SGLT2 and DPP4 inhibitor use. We estimated the propensity score for SGLT2 inhibitor users using a logistic regression model. To estimate the propensity score, we included the following variables: age, sex, BMI, waist circumference, systolic blood pressure, diastolic blood pressure, fasting plasma glucose, HbA1c, low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, triglycerides, AST, ALT, γ-GTP, cigarette smoking, alcohol consumption, physical inactivity, diabetic nephropathy, diabetic retinopathy, diabetic neuropathy, use of medications (insulin, glucagon-like peptide-1 receptor agonist, biguanide, sulfonylurea, α-glucosidase inhibitor, thiazolidine, glinide, renin-angiotensin system inhibitor, β-blocker, calcium channel blocker, mineralocorticoid receptor antagonist, diuretics, and statins), year of SGLT2 or DPP4 inhibitors prescription, and FLI at the initial health checkup. We matched SGLT2 and DPP4 inhibitor users using a 1:1 matching protocol (caliper width equal to 0.2 standard deviations of the logit score).
Outcomes
Outcomes were obtained from the annual health checkup data between 2005 and 2022. The primary outcome was the change in FLI after the initiation of SGLT2 or DPP4 inhibitors. The secondary outcomes were changes in γ-GTP, AST, ALT, BMI, waist circumference, and HbA1c levels. We followed the study participants for a maximum of 5 years after the initial health checkup.
Statistical analysis
The median (interquartile range) and number (percentage) were used to report descriptive statistics. We used a linear mixed-effects model for repeated measures with random intercept and slope, assuming an unstructured covariance structure, to compare the change in outcomes, including FLI, γ-GTP, AST, ALT, BMI, waist circumference, and HbA1c, among SGLT2 and DPP4 inhibitors. This model included the treatment group (SGLT2 or DPP4 inhibitors), time, and interaction between the treatment group and time. To examine the difference in the outcome changes among SGLT2 or DPP4 inhibitors, the P-value for the interaction between the treatment group and time was tested using Wald test.
If a significant difference in the primary outcome change was detected between SGLT2 and DPP4 inhibitors, we compared the change in FLI between individual SGLT2 inhibitors to examine whether the effects of SGLT2 inhibitors would be considered a class effect. We also performed a linear mixed-effects model for repeated measures to compare the change in FLI among empagliflozin, dapagliflozin, canagliflozin, ipragliflozin, tofogliflozin, and luseogliflozin. Presently, these six SGLT2 inhibitors are commercially available in Japan.
This model included individual SGLT2 inhibitors, time, the interaction between the individual SGLT2 inhibitors and time, age, sex, BMI, waist circumference, systolic blood pressure, diastolic blood pressure, fasting plasma glucose, HbA1c, low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, triglycerides, AST, ALT, γ-GTP, cigarette smoking, alcohol consumption, physical inactivity, diabetic nephropathy, diabetic retinopathy, diabetic neuropathy, use of the following medications (insulin, glucagon-like peptide-1 receptor agonist, biguanide, sulfonylurea, α-glucosidase inhibitor, thiazolidine, glinide, renin-angiotensin system inhibitor, β-blocker, calcium channel blocker, mineralocorticoid receptor antagonist, diuretics, and statins), and year of SGLT2 inhibitor prescription. To examine the difference in outcome changes among individual SGLT2 inhibitors, the P-value for the interaction between individual SGLT2 inhibitors and time was tested using a Wald test.
Three sensitivity analyses were performed to validate the primary findings. First, we examined the changes in FLI only in individuals who continued to use SGLT2 or DPP4 inhibitors for > 3 months. Second, we performed a linear mixed-effects model using a restricted cubic spline function with 4 knots to confirm the shape of the change in FLI from the initiation of SGLT2 inhibitors or DPP4 inhibitors. Third, we performed subgroup analyses stratified by age (≥ 50 and < 50 years), sex, BMI (≥ 30 and < 30 kg/m2), and HbA1c level at the initial health checkup (≥ 7.5 and < 7.5%). All statistical analyses were performed using STATA version 17 (StataCorp LLC, College Station, TX, USA).


Comments (0)