
Remember me
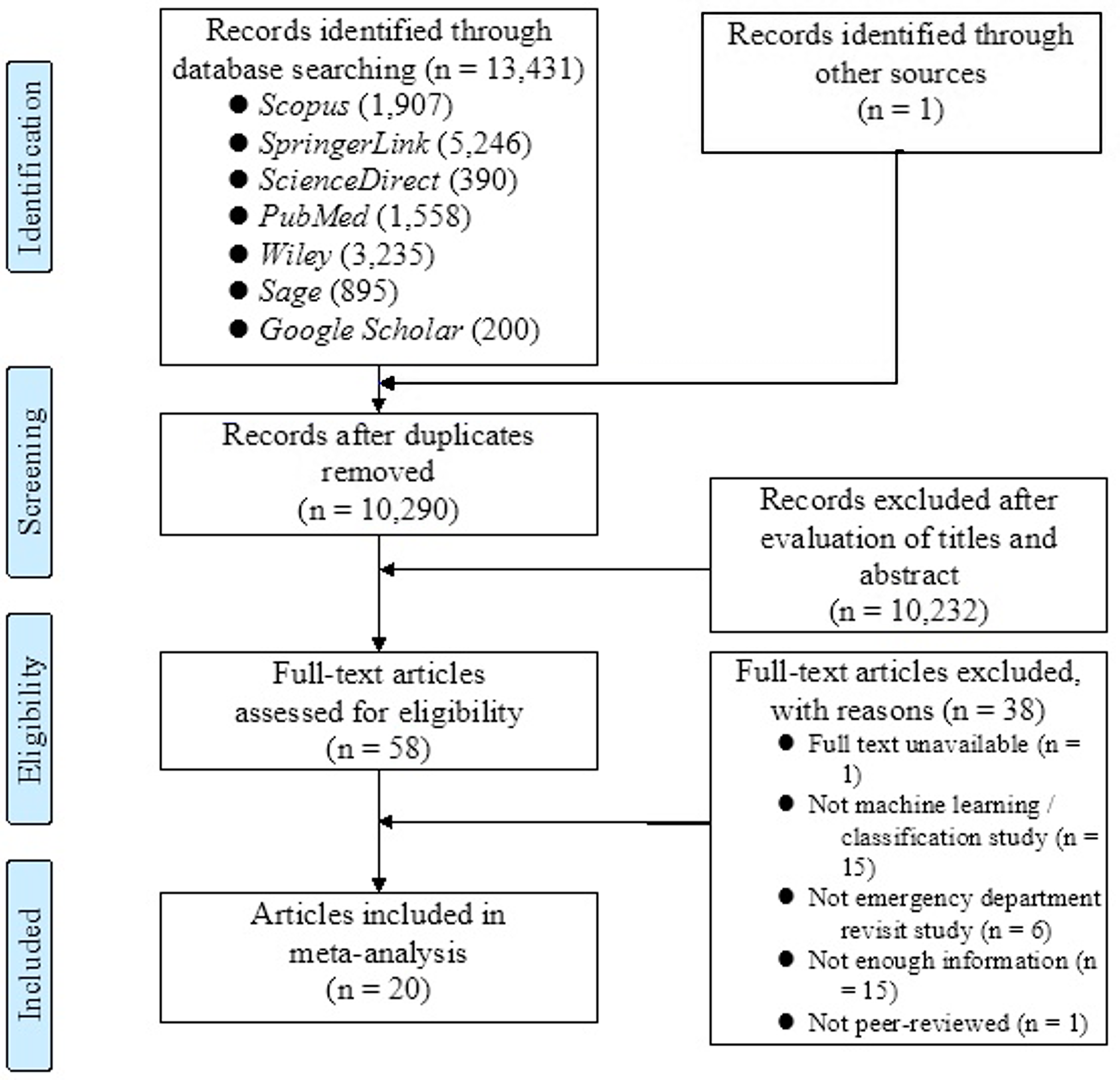
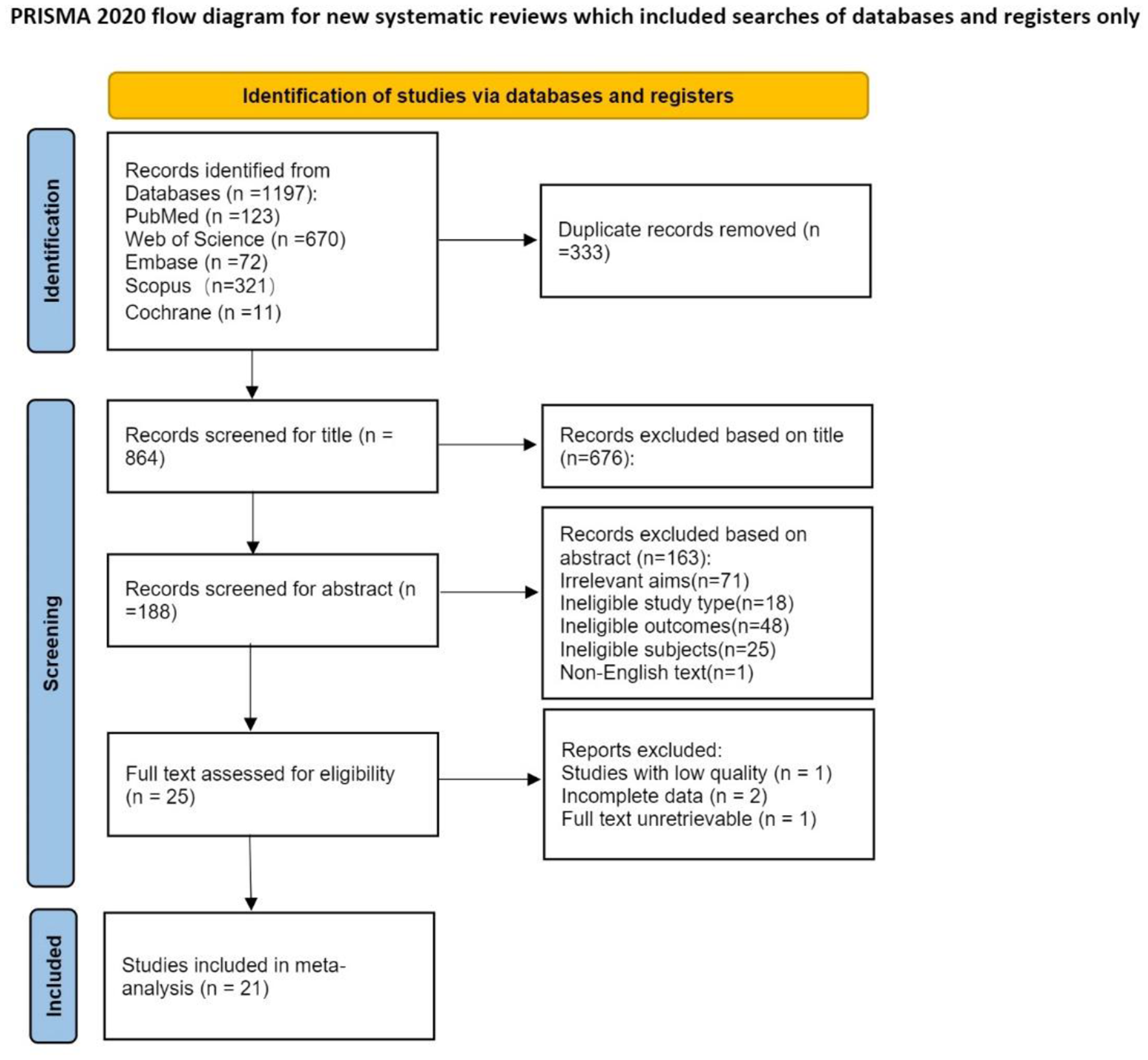
1227 articles were identified through database searching. After the elimination of duplicates, 1120 were collected by title and abstract. 87 records were assessed for eligibility, but only 12 met the inclusion criteria (Fig. 1) [18,19,20,21,22,23,24,25,26,27,28,29].From the reference lists, six relevant studies that evaluated and provided more information about four of the e-MedRec tools were identified [30,31,32,33,34,35].
Fig. 1
Study selection flowchart. MedRec, medication reconciliation
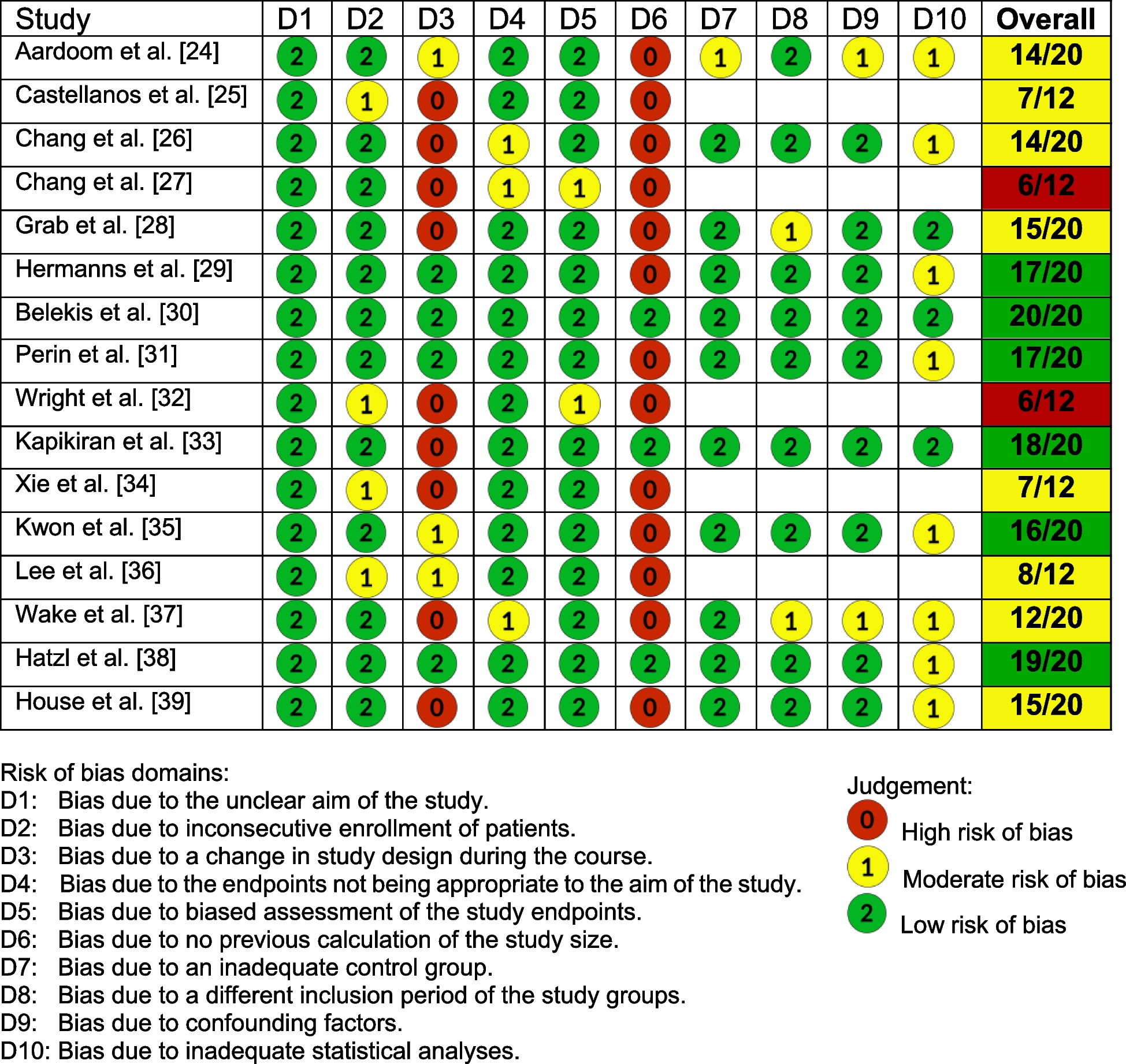
A quality assessment of the 12 selected studies was carried out. For QIPs, there was wide heterogeneity in the reporting criteria between studies, with some aspects of the available evidence or the purpose of the project being well documented, although ethical considerations were lacking in the majority of the studies. For RCTs, the items with the highest reporting rate (> 90%) were: title and abstract, background and eligibility criteria for participants, while the least covered standards (< 10%) were: changes to trial outcomes after the start of the trial or performing subgroup analyses. Finally, the observational study met most of the criteria, but potential sources of bias were not addressed.
The main characteristics of the studies which were included in the systematic review are summarized in Table 1. Six of the 12 studies were published over the last 10 years and two after 2020. Most studies were carried out in the USA (8), two were in Canada and only one in Belgium and Spain. With respect to study design, 8 were QIPs, 3 RCTs and only one was an observational study. Most transition points of care investigated were admission and discharge (2), discharge (4), outpatients (4) one in admission, transfer, and discharge (1), and the remaining one in admission (1). Four studies had no restrictions on eligible patients and no data were found in three. Test patients were included in one study [28].
Table 1 Description of the functionalities of the e-tools and their clinical impact on reconciliationTable 1 also shows the description of e-MedRec tools including the data entry, availability, and clinical impact on patient safety. Four e-tools [23, 26, 27, 29] could retrieve automatically information related to patients and their medication from community-drug lists, electronic medical records (EMR), or computerized provider order entry systems. One e-tool [18] allowed users to manually introduce the patient medication list or retrieve the last updated prescription from multiple electronic sources. Concerning the availability of the e-MedRec tools, all of them were computerized (software [18,19,20,21,22,23,24, 26, 28, 29] or website [25, 27]. “MedRec view” [19] was a commercially available software. Some of the software were embedded throughout EMR products such as Eclipsys Corporation [19], Siemens [22], Leapfrog [28], and EpicCare [29].Two tools were developed and provided by “Partners HealthCare System” [18, 20]. Two tools [20, 27] were created as a software prototype to incorporate into the EMR.“Twinlist” [19] was the only open-source website. The “MedRec web-app” [27] was a web application link available for all clinicians who have access to the Regional eHealth network with a mandatory log-in and secure password. No e-MedRec tool was implemented as a mobile app, but, clinicians who used the “MedRec web-app” [27] were interested in the adoption of the e-tool to be usable on smartphones and tablets. For the clinical impact of e-tools, some of them showed a reduction of medication errors, discrepancies, and adverse drug events among intervention patients compared to the usual care. However, no significant differences in emergency room visits or hospital readmissions were found with the use of “The RightRx Project” [26, 35].
Different functionalities were implemented in the e-tools to make the MedRec process more productive. Some examples are: displaying and comparing different medication lists ordered in columns to easily identify medication errors [19, 24,25,26,27, 29], transferring information between healthcare professionals [20, 26, 27], or grouping medicationsin different categories (therapeutic class, diagnosis, dosage, or ordered by clinical importance) [18, 25, 27]. Additional features were giving information to users about drug allergies or drug interactions [23] or clicking a button to continue, change or stop a medication [24, 26, 27]. Only the¨RightRx Project” [26] was able to generate a conciliation report that can be printed and given to patients once the medication list was updated. This tool was also the first to incorporate a data warehouse with a register of patient medication, prescribers, and dispensing pharmacies into the app. Additionally, a summary of the reconciled medication list in a “patient-friendly” language that could be printed and given to the patients might be included in the next prototypes of the “MedRec web-app”. Moreover, the authors of this application tested the opinion of users at various stages to obtain a sophisticated tool as a final product [27]. Color codes were implemented in the “Twinlist” [25] and “MedRec web-app” [27] to facilitate the MedRec process by healthcare professionals. Moreover, four tools were capable of triggering alerts or reminders to the providers related to medication discrepancies in order to enhance patient safety [19, 21, 24, 28].
The users' quality assessment of e-MedRec tools was evaluated in Table 2. Firstly, the majority of tools were aimed at physicians and pharmacists (6) while others could be used by physicians, pharmacists and nurses (3), physicians (2), and the remaining one was aimed at physicians, pharmacists, nurses, and patients. With respect to adherence, some authors measured the percentage of clinicians who used the e-tools [19, 21, 22, 27, 29] but others showed the number of medication lists updated by clinicians among patients [28]. Usability was measured by the reduction in time of MedRec process using the tool [18, 19, 25, 26], improvement in clinician workflow [22, 24], or patient safety [22, 28]. Clinician surveys were mainly used to assess satisfaction with the tools [18, 22, 29]. Finally, most of the users’ suggestions were aimed at the integration of the e-tool with the ordering process [18, 19, 27], interoperability [19, 27], and easier ways to reconcile the medication list [18, 19, 21, 26,
Comments (0)