
Remember me
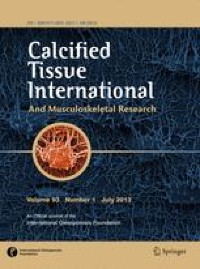

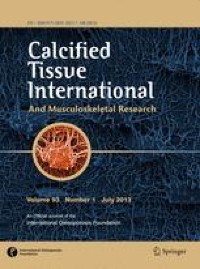

A total of 31 patients were identified with the referral diagnosis of CNO. After reviewing the medical records individually, 7 patients were excluded due to having another diagnosis than CNO of the jaw. Of these seven, 2 instead had CRMO, 2 were miscoded (they had osteoporosis instead), 1 had osteonecrosis (possibly secondary to Denosumab-treatment), 1 had trigeminal neuralgia, and 1 had pain remission with intensive dental surgery before initiating treatment at our site (diagnosis unknown). Thus, a total of 24 patients were included for further analysis. Patient inclusion in the study can be seen in Fig. 2.
Fig. 2
Flowchart of patient inclusion in the study
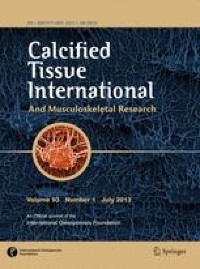
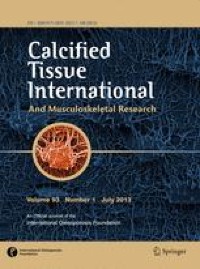
Anthropomorphic data on the 24 included patients are listed in Table 1. Of the 24 patients included, 15 had been discharged from the clinic by the end of the data collection period on March 1, 2023, while 9 were still being followed. A summary of the diagnostic tests used to verify the diagnosis can be seen in Fig. 3.
Fig. 3
Summary of the diagnostic tests used to confirm the diagnosis of CNO prior to referral
The average observational period was 33.4 months (median 23.0; Q1 11.5; Q3 42.0).
Patients were initially re-evaluated after the first the first dose of zoledronic acid, either by phone or by physical check-up, after an average of 4.3 months (median 3.5; Q1 1.9; Q3 4.8).
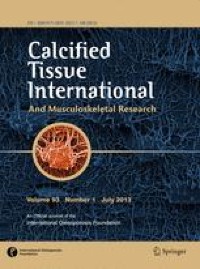
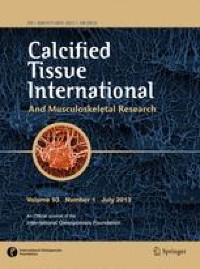
The average number of infusions of zoledronic acid given was 4.1 (median 3; Q1 2; Q3 5). The total number of doses of zoledronic acid given in the first 12 months can be seen in Fig. 4.
Fig. 4
Number of doses of zoledronic acid given within the first 12 months, including initial dose
No other treatment than zoledronic acid was given to the patients at the outpatient clinic. As seen in Table 1, patients had received a median of 2.5 months of antibiotical treatment prior to referral. We have no data on concomitant use of painkillers, either as prescription or over-the-counter use.
Blood tests were available for some patients (n = 17) from before receiving the first dose of zoledronic acid (baseline) and/or from the end of treatment (final follow-up).
P-CTX deceased significantly from baseline (median 443 ng/L (normal ref. value 125–1477 ng/L) to final follow-up (median 101 ng/L)(rank sum test; p < 0.001), while p-alkaline phosphatase did not change from baseline to follow-up (rank sum test; p = 0.393).
At least 67% of patients had at least one recurrence of pain after the first documented effect of zoledronic acid, and most experienced the first recurrence within 12 months after being given the initial dose of zoledronic acid (Fig. 5).
Fig. 5
Overview of patients’ 1st recurrence of CNO-related pain. N/A denotes insufficient records data to conclude whether a recurrence had occurred. This was mainly due to insufficient follow-up time (less than 12 months of follow-up)
Treatment effect, based on the pain reported by the patients, was recorded after 12 months and at final discharge from the clinic (Fig. 6). Twelve months after initiation of treatment, 71% of the patients reported either no pain or reduced pain.
Fig. 6
Pain relief after treatment with zoledronic acid
At final discharge, or end of data collection, 46% of the patients reported no pain and a further 38% had a reduced pain.
Treatment effect was also evaluated by imaging diagnostics in 10 patients (SPECT/CT or bone scintigraphy). Of these 10 patients, 6 had no activity in the jaw area with CNO, 2 had reduced activity, and 2 had unchanged activity. Reduced activity was not uniformly related to pain, as 1 patient with no imaging activity still had unchanged pain, while another patient without any pain still had unchanged activity. Of the rest (n = 8), 4 had no imaging activity and reduced pain, 2 had reduced imaging activity and reduced pain, 1 had reduced imaging activity and no pain, and the last patient had unchanged imaging activity and unchanged pain.
A total of 4 patients (16%) had unchanged pain after treatment with zoledronic acid and were thus recorded as such by the end of data collection. They had all been discharged from the clinic due to lack of treatment effect before the date of March 1, 2023. The group consisted of 3 females and 1 male, had received an average of 2 doses of zoledronic acid (range 1–3), and had been followed for an average of 6.8 months (Table 2).
Table 2 Comparison of responder versus non-respondersThere were no significant differences between responders and non-responders regarding gender, age, duration of symptoms prior to treatment, or number of infusions with zoledronic acid given.
Data from Follow-Up Phone InterviewWe were able to reach 20 out of the 24 patients for a follow-up interview by phone.
The average VAS score, as evaluated at the final phone interview, dropped significantly from 7.7 (1.5 SD; median 8; range 5–10) before treatment to 2.5 (2.3 SD; median 2; range 2–7.5) at final discharge or end of data collection (p < 0.001, signed rank test).
Patients (n = 20) were asked whether they still felt any discomfort from their jaw in the form of intermittent throbbing (n = 9), intermittent pain spikes (n = 9), and/or reduced function (n = 7; 3 of whom had had no effect of the treatment). Patients were also asked if their jaw or face had altered its appearance in their own perception (n = 2). Three patients had no symptoms remaining at all.
Comments (0)