
Remember me
Thanks to an international collaboration we identified altogether five families with different PLS3 variants leading to EOOP in one or more family members. We describe the clinical features of the five index patients and the genetic variants identified in altogether ten mutation-positive individuals. The data are also summarized in Table 1.
Table 1 Clinical characteristics, fracture history, BMD scores at the time of first evaluation from the index patients of five families with a pathogenic variant in the gene encoding plastin-3 (PLS3)Family 1The proband is an 8-year-old Swedish boy referred for investigation due to multiple low-energy fractures. At 2 years of age, he had his first fracture after minimal trauma. By 8 years, he had had eight fractures after minor trauma (ulna, radius, humerus, tibia, and metacarpals).
He is the fifth out of six children of healthy European parents and had an unremarkable neonatal and childhood period. None of the parents have a history of skeletal disease. The patient’s maternal uncle, age 38 years, has a history of multiple fractures and severe back pain requiring analgesic medication since young age (Fig. 1), having a clinical diagnosis of Osteoporosis pseudoglioma syndrome since 11 years old.
Fig. 1
Families pedigrees: Pedigrees of the five families presented with mutation of the PLS3 gene
On physical examination at 8 years, the proband’s height was 142.5 cm (+ 2.0 SD) and body mass index (BMI) 17.9 kg/m2 (+ 1.0 SD). He had pectus excavatum, flat feet, broad and short thumbs and digits 4–5 syndactyly bilaterally. Dental examination with radiography showed poor trabecular bone in the jaw bone, but was otherwise normal.
The BMD measurements showed a Z-score of − 1.6 at lumbar spine (LS). Spine x-ray showed reduced height (approximately 40%) of T5 and slightly wedged vertebral bodies C3–C5 (Fig. 2A).
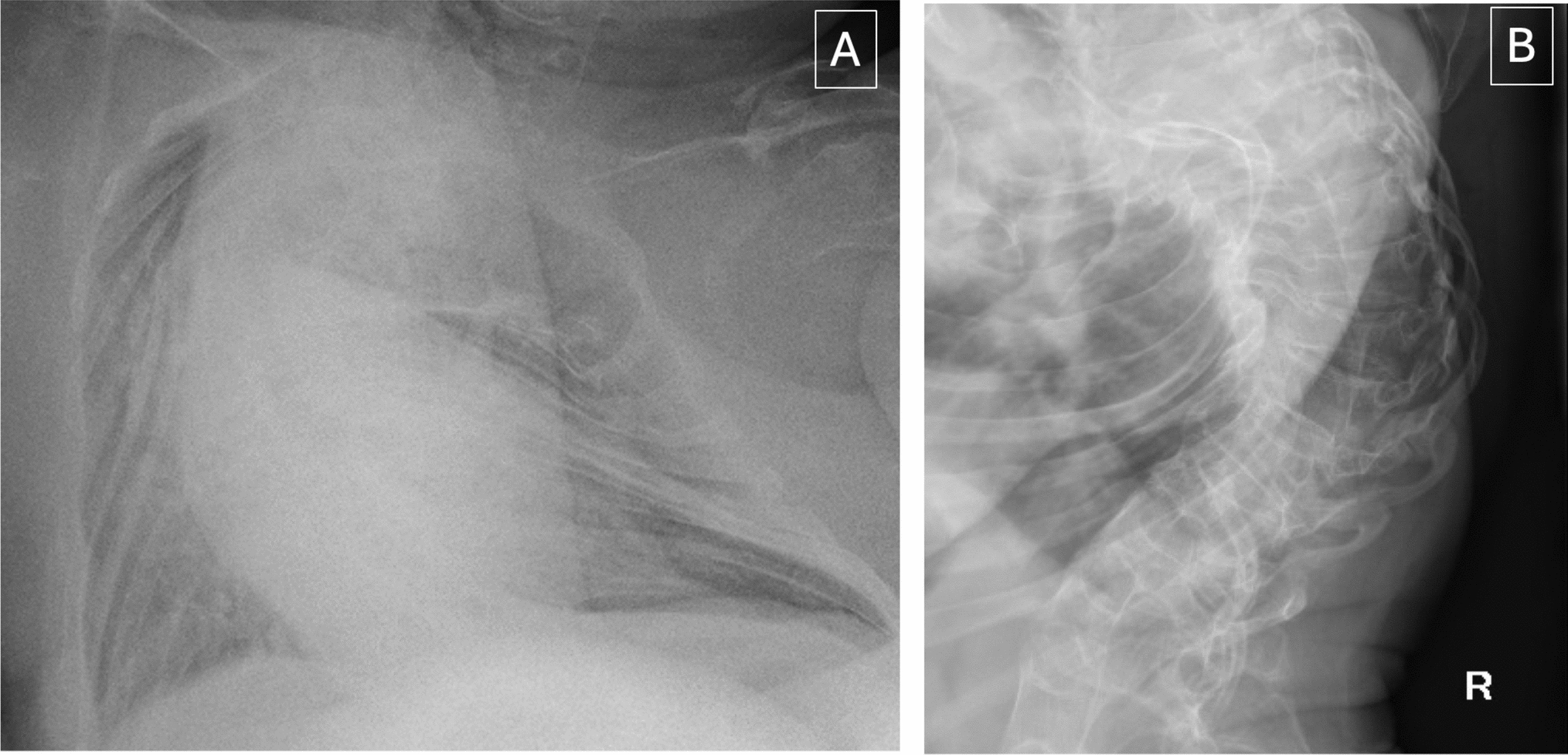
Fig. 2
Spinal images: collapse and a reduction of height of multiple vertebral bodies: A Family 1 index patient’s x-ray; B Family 2 index patient’s CT; C Family 3 index patient’s MRI; D Family 4 index patient’s MRI; E Family 5 index patient’s MRI
Genetic analysis with a gene panel (Blueprint Genetics) identified a hemizygous frameshift variant in PLS3 [c.1543del (p.Asp515Metfs*11)] in the proband (Fig. 3). This variant was classified as likely pathogenic and was inherited from the unaffected mother who also harbored the same PLS3 variant. This variant is predicted to cause loss of normal protein function through protein truncation and/or nonsense-mediated mRNA decay. The variant is absent in gnomAD and has not been described in the medical literature or reported in any disease-related variant database. The DNA sample of the mother’s brother, who also had osteoporosis, was not available for testing.
Fig. 3
PLS3 variants: Schematic representation of PLS3 the RNA-splicing form NM_005032.6 showing the location of the 5 identified variants. E1-16 = exons 1–16
The patient has been treated with bisphosphonates (pamidronate monthly) for the last 10 months and has not experienced any new fractures during this period.
Family 2This 26-year-old European man was referred due to unstable fracture at L1 vertebra after a low impact trauma, managed with posterior spinal fusion (Fig. 2B). He had a past history of radius fractures, at the age of 13 and 15 years, following sports injury. The physical examination was unremarkable (height 162 cm − 2.0 SD, BMI 23 kg/m2 + 0.5 SD).
He was born from healthy non-consanguineous parents. There was a family history of multiple fractures in his grandfather and his uncle, from his mother’s family arm (Fig. 1).
The BMD Z-score (GE, Lunar Prodigy Pro) at the LS was − 3.7. BMD measurements of the family members revealed that his brother, aged 20 years, had low BMD at LS (Z-score − 3.1), FN (Z-score − 2.4), and Radius 33% (Z-score − 3.0). His father had osteopenia at LS (T-score − 2.3) and FN (T-score − 1.5). His sister aged 21 years and his mother aged 46 years had normal BMD, LS Z-score − 0.8 and − 1.7, respectively.
Sanger sequencing revealed a novel nonsense variant in PLS3, c.827G>A (pTrp276T*), in the index case (RefSeq NM_005032) (Fig. 3). This variant was maternally inherited and the index’s brother also harbored the same variant.
The proband was started on teriparatide treatment along with calcium and vitamin D. Ten months after teriparatide, BMD Z-score of the FN was − 2.8 and TH − 2.7, increased by 2.4% and 4.1%, respectively, while radius BMD did not change. BMD at LS (0.579 g/cm2/ Z-score − 5.1) decreased by 22%. No fractures or adverse events occurred during the 10-month follow-up. One possible explanation for the substantial decline at the LS (as opposed to the improvement at the hip) is the trajectory of BMD following spinal fusion surgery. Indeed, 5 months later, BMD at the LS increased by 5.7% (Z-score − 4.9).
Family 3The patient is a now 20-year-old man, the only child of a healthy non-consanguineous couple of Russian descent. The parents are of average height without a fracture history (Fig. 1). He presented to pediatric endocrinology at the age of 7 years for evaluation of short stature. At that time, he had suffered a finger fracture after a fall, at the age of 5 years, followed by a fracture of the left femur and of the right tibia due to minor falls. A diagnosis of growth hormone (GH) deficiency was established based on insufficient GH levels in two GH stimulation tests at 9 years of age and he was started on recombinant human GH. GH treatment was discontinued at 17 years when the annual growth rate fell below 3 cm. The final height is 176 cm (− 0.6 SD), which falls in the range of the parental target height and he developed a mild pectus carinatum.
BMD by DXA at 9 years revealed a Z-score of − 2.8 at the LS. Following the initiation of GH therapy, the Z-score improved to − 2.5 at age 13, but at 16 years, the Z-score had dropped to − 2.9. Magnetic resonance imaging (MRI) revealed collapse of multiple vertebral bodies (Fig. 2C).
Genetic testing showed an X-linked inherited osteoporosis caused by a hemizygous mutation in the PLS3 gene [c.994_995delGA (p.Asp332*)]. This diagnosis was established at the age of 18 years (Fig. 3).
Treatment was started with vitamin D and calcium supplementation and intravenous bisphosphonate (pamidronate). In the 1st year he only received 3 mg/kg body weight of pamidronate. It was intended to administer 9 mg/kg BW for the 1st year. However, due to the onset of the coronavirus disease pandemic in 2020 the follow up visits had to be canceled. Treatment was switched to zoledronate and he received two doses of 4 mg in 6 months’ intervals. At 18 years (after the low dose of pamidronate), the LS BMD had mildly improved with a Z-score − 2.6. At the same time an X-ray of the spine showed normal height of the vertebrae of the thoracic and lumbar spine. During follow-up no fractures occurred.
Family 4The index patient is a currently 17-year-old adolescent of Polish descent treated for X-linked juvenile osteoporosis and a pectus carinatum in the endocrine and bone health clinic of a tertiary university hospital. His height is 170.7 cm (− 1 SD) and the BMI is 17.8 kg/m2 (− 2 SD).
The first fracture occurred at the age of 1.5 years and by 8 years of age, six additional fractures (forearm, wrist, elbow -twice- and clavicle) had occurred. At 13 years of age a fall resulted in a vertebral fracture of L2, which required spinal fusion surgery (Fig. 2D) and he was presented to a specialized bone clinic for suspected OI. Physical examination revealed marked hypermobility of the joints and a mild thoracic asymmetry.
Family history revealed back pain in the mother, but fractures had never occurred. The patient's maternal grandfather had suffered from fractures sporadically, but due to adequate trauma. The patient has a healthy sister (Fig. 1).
A DXA scan at 12 years revealed a LS Z-score of − 2.9. A follow up at age 13.5 years showed a Z-score of − 3.0 after the osteosynthesis material was removed. Molecular genetic testing revealed a hemizygous deletion starting before the PLS3 gene and spanning into intron 3 of the same gene (chromosomal coordinates X:114771600-114890428) (Fig. 3). Genetic testing of the mother revealed that she is a heterozygous carrier of the deletion (DXA with LS T-score of − 1).
Due to the multiple fractures and reported back pain an intravenous therapy with pamidronate (9 mg/kg BW in the 1st year, 5 mg/kg BW subsequently) was started at the age of 13.5 years. A thoracic x-ray at age 15.5 years showed a loss of height at thoracic vertebra Τ12. The corresponding DXA measurement revealed a LS Z-score of − 3.5 (− 2.7 after adjusting for height). Even though the DXA Z-score did not improve with the therapy, there have been no further fractures since the treatment with bisphosphonates was started.
Family 5An 11-year-old Portuguese boy, the only child of a healthy Portuguese couple (Fig. 1), has a past history of two finger fractures after a sports injury at the age of 8 years and obesity. At 11 years-old, he was 144.9 cm tall (− 0.07 SD) with a weight of 60.9 kg (+ 2 SD) and BMI of 29 kg/m2 (+ 2 SD). He was admitted to the hospital due to a 3-month progressive worsening of lumbar pain with increasing difficulty to walk due to multiple spinal fractures. There was no history of trauma. The physical examination was unremarkable. His 36-year-old father had lumbar spine osteoporosis but no fractures. The mother is healthy, has no history of bone fractures and has a normal BMD.
An MRI of the spine revealed multiple vertebral body fractures (from C7 to L5, only sparing T1, T2, T10, and L1) with collapse and a height reduction of 25–50% (Fig. 2E). Full body X-ray scan revealed diffuse osteopenia but did not find any other fractures. The DXA revealed a Z-score of − 5.0 in LS. Neurological, cardiological, ENT, and ophthalmological evaluations were normal.
Next-generation sequencing (Illumina) of genomic DNA for 26 genes, including PLS3, was performed (Human All Exon V6, Agilent Technologies) and led to the identification of a novel hemizygous deletion removing the whole PLS3 gene (Fig. 3). Array comparative genomic hybridization, CytoScan 750 K, confirmed the presence of a 775 kb deletion on chromosome X (coordinates X:114644041-115418576) removing the entire PLS3 gene as well as AGTR2, encoding type-2 angiotensin II receptor.
A heterozygous variant of unknown significance (VUS) in LRP5 was also identified [NM_002335.3:c.3443C>T(p.Thr1148Ile)]. The patient inherited the PLS3 deletion from his unaffected mother and the LRP5 variant from his father with spinal osteoporosis but no fractures.
The patient started quarterly intravenous pamidronate cycles (1 mg/kg/day for 3 days), calcium and vitamin D. After 1 year of treatment the DXA revealed a general increase in all BMD values (Z-score + 0.7 in LS) and regression of all symptoms, with no new fractures.
Comments (0)