
Remember me
For the present study, we evaluated a new navigation system enabling augmented AR-supported pedicle screw placement while integrating navigation cameras into the reference array and drill guide. The clinical application of the image-guided navigation system was feasible in multiple indications, such as trauma, degeneration, infection, and tumor. Pedicle screw placement was performed in open and in percutaneous technique, and navigation was precise in both techniques. Additional cement augmentation of the cannulated pedicle screws was performed in 50% of cases.
In all cases, navigated pedicle screw placement could be performed successfully, while intraoperative imaging had to be repeated in 15% of the cases due to insufficient imaging data, and in one case, a delay related to software issues (5.0%) was reported. With a focus on accuracy and patient safety, 90.5% of pedicle screws were rated GRS Grade A or B (Fig. 3), with a rate of screw revisions of 1.7% in this study. No new neurological deficits postoperatively. In a large study performed by Ille et al. [11] analyzing the accuracy of navigated pedicle screw placement in 6733 pedicle screws of the whole spine, an overall rate of screw revision of 3.4% was observed. Another study conducted by Ryang et al. [9] in 2011 and 2012 on navigated pedicle screw placement reported a screw revision rate of 4.7% for lumbar pedicle screw placement. These results match with studies performed by Waschke et al. reporting accuracy rates of 96.4% in CT-navigated pedicle screw placement, and Tkatschenko et al. showing accuracy rates of 96.6% for navigated percutaneous pedicle screw implantation [7, 22].
In this study, the duration between skin incision and first intraoperative imaging was 19 ± 11 (9–40) min, and the estimated duration per screw was 6.5 ± 1.9 (4.0–11.5) minutes. A comparable study by Ding et al. on navigated pedicle screw placement measured a time of skin incision to reference frame attachment of 28.3 ± 20.4 min and a time of 7.8 ± 2.7 min for a single pedicle screw placement [23]. The average time required from skin incision to reference frame attachment was 28.3 ± 20.4 min, and the average time required for insertion of a single pedicle screw was 7.8 ± 2.7 min [23]. Durations of pedicle screw placement on the thoracolumbar spine as low as 3.9 ± 2.5 (1–22) min were reported by Ryang et al. [9]. However, this report measured the time from placement of the navigated drill guide on the supposed/ planned pedicle entry point to final pedicle screw insertion [9].
Regarding radiation dose, comparable settings for ORCT or 3D C-Arm imaging were applied compared to spinal navigation systems routinely applied at our institution. This results in a similar radiation dose, in total as well as per pedicle screw.
Canulated pedicle screws of titanium, as well as titanium rods, were used in this study. No intraoperative case of hardware failure was reported. One implant failure (loosened pedicle screw nuts) occurred in a long-segment construct.
Intraoperative set-upConventional CT-based spinal navigation systems applied in clinical routine mostly require a setup consisting of a central computing unit, display units and an external adjustable infrared camera [9, 11]. In many cases, the system is permanently installed in the operation room. Furthermore, a device for intraoperative 3D imaging, including software integration to the navigation system, is required. To provide intraoperative navigation, a reference array has to be attached to the patient, and all surgical instruments have to be equipped with reflective marker spheres.
In contrast, the system applied in this study offers excellent versatility. As the reference array is equipped with targets incorporating LEDs and any navigated instrument is equipped with a camera, there is no need for an external infrared camera constantly being placed in the field of vision of reflective markers (Fig. 1). This enables improved visibility of the reference array without the necessity to adapt camera positioning due to line-of-sight issues [24]. Furthermore, only one main computing unit compact in size and equipped with a single screen is required (Fig. 5). Overall, the setup is reduced to a minimum by integrating the cameras into the surgical instruments and establishing a flexible platform, including preoperative planning. No specific modifications of the operating room or the 3D-imaging device, such as installing a reference frame, are required. This results in great flexibility and enables a versatile application of the system in multiple operation rooms as well as for several indications reaching beyond the instrumentation of the spine. However, the targets incorporating LEDs and cameras are single-use materials and are required for every surgery.
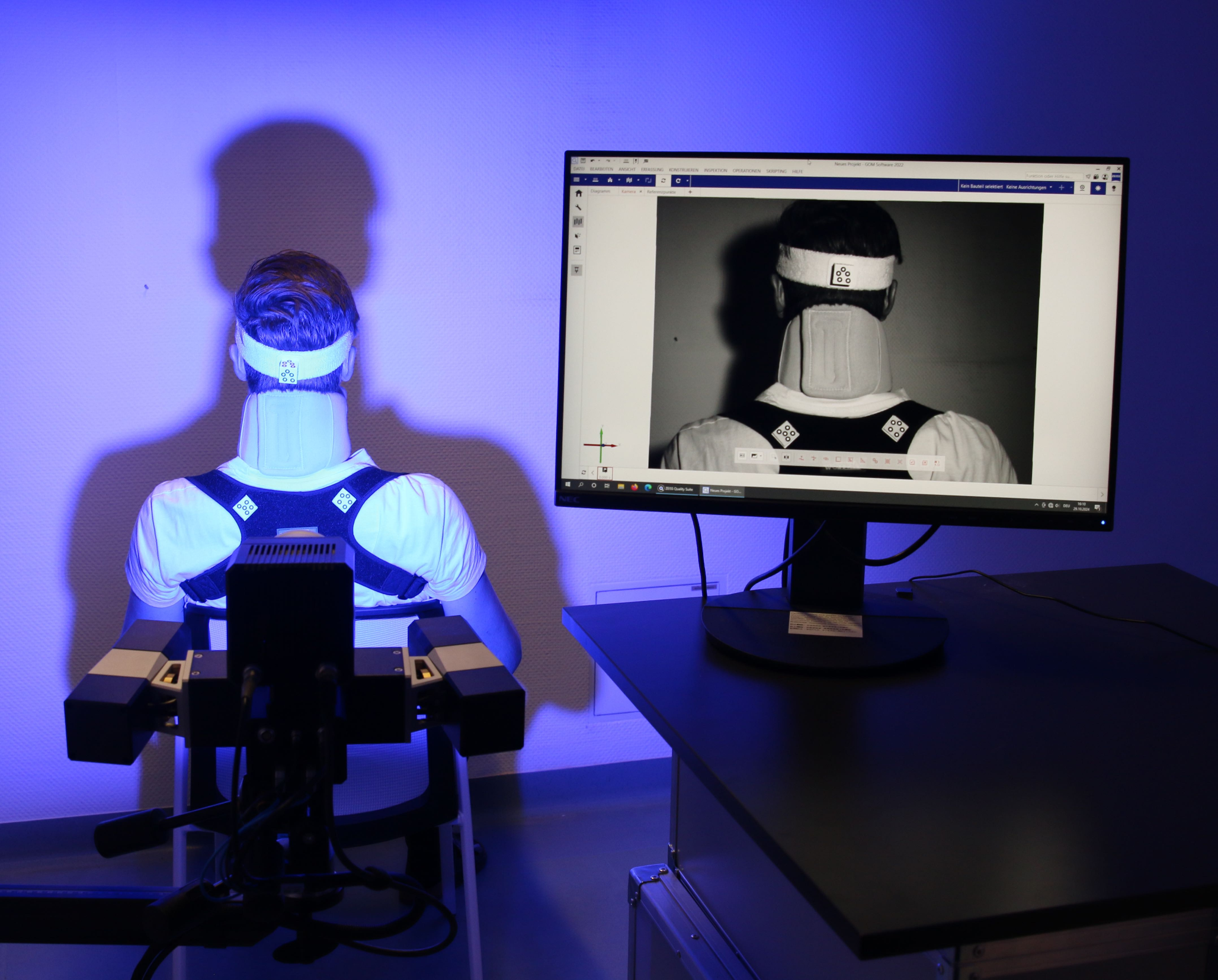
Fig. 5
Complete setup. Figure 5 represents the complete setup of the system required for spinal navigation. The mobile main computing unit (left) is equipped with a single screen. Furthermore, the sterile system (right) consists of two targets attached to the reference array and a camera attached to the surgical instruments, such as the navigated drill guide shown in this figure
Intraoperative addition of augmented realityThe system offers the option to apply AR intraoperatively. Intraoperatively, the 3D imaging is integrated into the navigation software enabling real-time planning of the pedicle screw positioning on an external screen or integrated into an augmented reality view. The view can be chosen by the surgeon individually and changed intraoperatively. AR goggles (NextAR Smart Glasses, Medacta, Castel San Pietro, Switzerland) present the 3D-imaging and neuronavigation data combined with the view of the operation situs (Fig. 2). Subjectively perceived, the fact that the surgeons' view has not been averted from the situs has been rated advantageously. In general, AR is constantly gaining increasing importance in surgery. Augmented reality in pedicle screw placement has become technically feasible over the last few years [13,14,15,16,17,18,19,20]. Recent studies in models and first clinical applications have shown promising results, especially regarding improved visualization of the situs, reduced time of surgery, and precise screw positioning [16, 25, 26].
LimitationsAs this study aimed to evaluate the feasibility of this novel navigation system enabling AR, this study was limited to 20 patients at one single high-volume spine center. As a result, no specific analysis regarding instrumentation using only AR was performed.
Comments (0)