The aim of this study was to evaluate and compare the immobilizing effects of a semi-rigid cervical orthosis against a soft and a rigid cervical orthosis on c-spine mobility, to determine whether it could serve as a viable alternative for c-spine immobilization.
Overall, while the rigid orthosis provides the most significant restriction of mobility, the semi-rigid orthosis demonstrates a significant difference in flexion and extension compared to the soft orthosis and provides a substantial movement restriction compared to the unrestricted ROM.
Evaluating c-spine motion is challenging due to its complex anatomy and combined movements. Traditionally, radiographic methods were used to assess spinal motion; however, these posed significant radiation risks [11]. Advances in non-invasive motion analysis techniques, including goniometry, inclinometry, and motion capture systems, have largely replaced them [9, 10]. In this study, motion tracking was implemented using a 3D camera system, an established method known for its high spatial and temporal resolution. Systematic reviews have identified marker-based 3D motion capture as the gold standard for clinical and biomechanical motion analysis, particularly for capturing spinal and rotational movements [13,14,15].
The obtained unrestricted ROM of the participants in this study aligns with normative medical data when measured using a 3D camera system [16]. Additionally, the ROM restrictions caused by the soft and rigid cervical orthoses in the present study are comparable to previously reported results [3, 12].
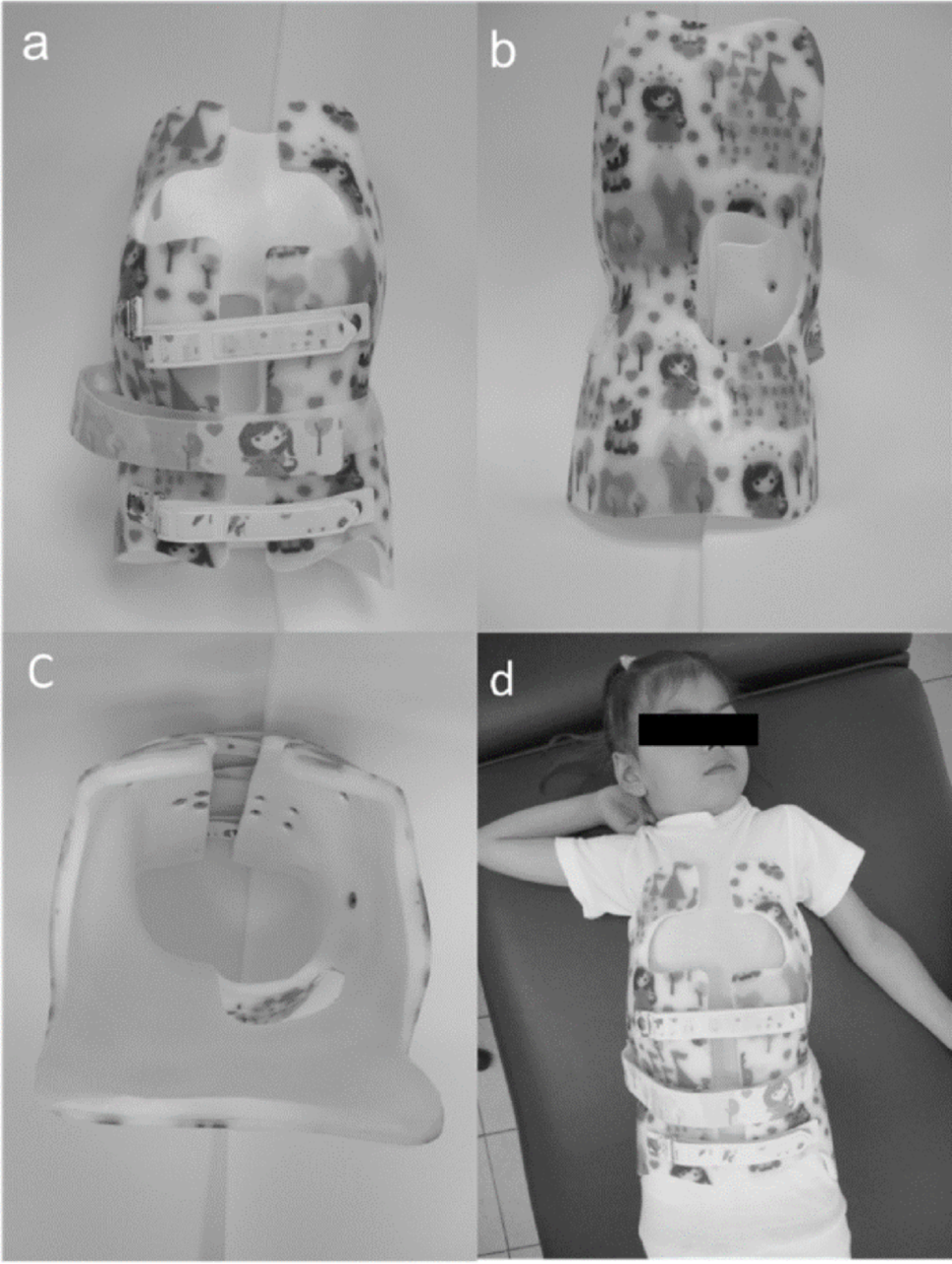
The differences in immobilization observed among the three tested cervical orthoses can be attributed to their structural design and material composition (see Supplemental Material for product descriptions). The rigid collar (Miami J Select, Oessur) consists of a firm anterior and posterior shell that provides maximum stabilization. In contrast, soft collars, such as Cervi-moll (Thuasne) are made of foam-based materials. Semi-rigid orthoses, such as the PDC brace (Thuasne), combine both rigid and flexible components, offering an intermediate solution. The results of this study align with these material properties, as the rigid collar provided the highest immobilization, followed by the semi-rigid orthosis, while the soft collar permitted more movement.
Across all three tested orthoses, the most movement restriction was observed in flexion/extension. Rotation was somewhat less restricted, and lateral flexion was limited the least. These findings align with previous studies on Type 1 cervical collars as classified by Johnson [3, 12, 17]. Biomechanically, this is explained by the primary stabilization points of these orthoses being ventral at the chin and thorax, and dorsal at the occiput and upper back, thus primarily acting in the sagittal plane.
Since previous research suggests that c-spine mobility may be influenced by factors such as age, gender, and body constitution, these demographic variables were recorded in this study (Table 1). Earlier studies reported an age-related decline in cervical ROM, likely due to degenerative changes [18], while more recent investigations have also identified gender-related differences in cervical mobility [19]. However, no existing studies indicate that these factors influence the immobilization effects of cervical orthoses [12, 20]. Consistent with this, the present study found no significant impact of gender, age, or BMI on the functional ROM restriction provided by the three tested orthoses.
Cervical orthoses remain a standard treatment for c-spine injuries. In clinical practice, depending on the type of injury, an orthosis must be selected that sufficiently restricts c-spine movement while minimizing complications such as pressure ulcers or breathing difficulties. The presented findings suggest that the use of a rigid orthosis and the potentially associated complications could be avoided, particularly after procedures involving internal fixation, because semi-rigid and soft collars seem to be sufficient for restricting motion during routine activities until the normal, physiologic ROM of the c-spine has been restored. However, for higher-grade unstable c-spine injuries, a semi-rigid or soft orthosis may still be insufficient [21]. It is critical to consider the established protocols, such as the NEXUS criteria and Canadian c-spine rules, to determine the need for c-spine immobilization, initiating timely imaging, and develop a management strategy based on diagnostic findings [22, 23]. Depending on diagnostic results, these approaches aid in either clearing the c-spine or initiating appropriate interventions, such as early surgical stabilization [24, 25]. Until stabilization is achieved, rigid cervical orthoses may still be necessary for immobilization despite their associated risks. Wherever possible, early transition to semi-rigid or soft collars should be prioritized to minimize these complications.
The presented findings support the hypothesis that the PDC, as a semi-rigid cervical orthosis, provides an intermediate option for c-spine immobilization. The PDC limits c-spine mobility, particularly in flexion/extension, offering a viable compromise between soft and rigid braces. While rigid orthoses provide the highest immobilization, according to literature, their use is often associated with higher complication rates, including pressure ulcers, dysphagia, and respiratory compromise [5,6,7]. Compared to soft collars, the semi-rigid orthosis showed a significantly greater restriction in extension and flexion, with a similar trend observed in other movement directions. No evidence suggests an increased complication rate with the semi-rigid collar compared to the soft collar. Based on these findings, semi-rigid orthoses may be a suitable alternative in clinical scenarios requiring c-spine immobilization.
Limitations of this study include that fact that blinding was not feasible for either the observer or the participants. However, participants were blinded to the results obtained with or without orthoses, and data were analyzed in a coded manner, ensuring that the test conditions were not known during analysis.
The subjective perception of orthosis deformation was used as the endpoint for movements. This subjective perception represents a potential limitation of the presented method. It can be assumed that, due to repeated movements by the same subject with all three orthoses, this potential error is at least consistently reproduced, allowing for reliable conclusions about movement restriction.
Another limitation of this study is that it was conducted on healthy subjects without spinal instability or neck pain. Nevertheless, the efficacy of the cervical orthoses is demonstrated in preventing complications arising from unintentional movements and secondary damage in patients with pre-existing conditions, pain, or movement restrictions in the c-spine.

Comments (0)