In sacral surgery, particularly sacrectomy, the primary objectives are to achieve R0 resection in oncologic cases and to completely eradicate infection in cases of infection. The existing literature supports that both R0 and, in certain cases, R1 resections confer a survival advantage in sacral tumors [9,10,11]. In our series, we successfully achieved R0 resection in 16 out of 18 patients. However, in one case involving a malignant mesenchymal tumor, we achieved R1 resection, and in a patient with sacral metastasis from thyroid cancer, R1 resection was also performed. Among the surviving patients, we observed a recurrence rate of 31% during a median follow-up of 41 months, which is consistent with published data. This recurrence rate can likely be attributed to factors such as the aggressive nature of the primary sacral tumors and the potential for microscopic seeding or metastasis at the time of surgery.
Our survival rate, which aligns with that reported in the literature, was 72%, reflecting our consistent aim of achieving R0 resection in oncologic surgeries and administering long-term antibiotic therapy in infectious cases [9,10,11]. Unfortunately, five patients in our series succumbed to their conditions. One patient with extensive malignant peritoneal mesothelioma (200 mm) passed away within the first month post-surgery. Another patient died about a month after intestinal surgery due to intestinal necrosis. While the exact cause of necrosis remains unclear, we speculate it may be related to fibrotic damage from the sacral surgery or circulatory complications stemming from the initial procedure. The remaining patients who died succumbed to hemorrhage approximately one month after surgery. Notably, the median tumor volume of the deceased patients was 1760 cm³, indicating an exceptionally large and advanced tumor burden.
Nerve root resection during sacrectomy significantly influences patient-reported outcomes, particularly concerning physical and mental health [12]. In our surgical approach, we prioritized preserving nerve roots as much as possible to minimize complications. However, our primary goal remained achieving R0 resection—complete tumor removal with clear margins. Despite these efforts, neurological complications were observed in 10 patients (55%), manifesting as varying degrees of sensory and motor deficits. Our findings align with existing literature, which highlights the significant impact of nerve root sacrifice on functional outcomes. Specifically, patients who underwent S2 or more proximal resections experienced a greater degree of neurological dysfunction, particularly regarding bladder and bowel control (8/9 cases). Prior studies have demonstrated that bilateral S2 resection leads to near-universal loss of sphincter control, while unilateral nerve root preservation may help retain partial function [13, 14]. Comparatively, literature reports indicate that normal bladder function is present in 25% of cases when one S2 root is spared, 39.9% when both S2 are spared, and 83.3% when both S3 are preserved. When even one S4 root is spared, bladder and bowel function are maintained in 100% of cases [12,13,14]. Our results corroborate these trends, reinforcing the critical role of the nerve root preservation level in determining functional outcomes following sacrectomy.
Wound site complications are a well-documented and significant challenge following sacrectomies, as they can negatively impact postoperative recovery and patient outcomes [15]. The incidence of such complications has been reported to be approximately 30% in the existing literature. However, our series revealed a notably higher incidence of around 50%, highlighting the need for closer examination of factors influencing wound healing in this specific patient group [16]. One possible explanation for this discrepancy is the reduced immunity observed in the elderly southeast European population, which may be less robust compared to their Western counterparts. This can be influenced by various socio-economic and healthcare factors that may lead to overall lower immune function. Additionally, factors such as poor nutritional status, underlying comorbidities like diabetes or cardiovascular conditions, and general health disparities between populations could contribute to the heightened vulnerability of these patients to postoperative complications [17]. It is crucial to recognize that these factors are not uniform across different geographical regions and that population-specific characteristics must be taken into account when assessing the risks of wound healing complications. Further research focused on these variables—such as the impact of regional nutritional habits, healthcare access, and the management of preexisting conditions—could provide valuable insights into optimizing care strategies for elderly southeast European patients undergoing sacrectomy. Such research may lead to more targeted interventions to improve outcomes and reduce complications in this population, ultimately enhancing the overall success of sacrectomy procedures.
In the context of surgical site infections, VRAM flaps showed a favorable outcome, with infection rates remaining comparable to those in the non-flap group, despite the increased complexity of the surgeries. Although flap procedures involved larger tumor volumes and longer operative times, the infection rates did not differ significantly between the VRAM and non-flap groups. Interestingly, patients who developed infections following VRAM reconstruction had shorter hospital stays compared to those in the non-flap group. This could be considered a positive outcome, suggesting that VRAM flap procedures may contribute to more effective management of infections, potentially leading to faster recovery. A possible explanation for this difference could be the types of infectious agents present: in the VRAM group, infections were predominantly caused by anaerobic bacteria and Escherichia coli, whereas in the non-flap group, infections were caused by Gram-negative, highly resistant bacilli like Pseudomonas aeruginosa and Acinetobacter baumannii. This difference in the microbial profile may explain the shorter recovery time in patients with VRAM reconstructions. This finding also suggests the potential for vascularized flaps to act as a defense mechanism against Gram-negative, resistant bacilli.
The management of SSI following sacrectomy is particularly challenging in cases with polymicrobial anaerobic infections. These infections are often severe and prolonged, requiring multiple rounds of debridement to control the infection and facilitate healing. Anaerobic bacteria commonly complicate wound management, leading to extended recovery times. Timely and aggressive debridement is essential for reducing bacterial load and preventing further complications. In cases with poorly vascularized tissues, the risk of polymicrobial anaerobic infections increases, making debridement even more critical. Our results demonstrated the positive impact of this approach, particularly in patients with weakly vascularized tissues and anaerobic infections. Based on our findings, we recommend repeated debridement as an essential part of managing these challenging cases to ensure more effective infection control and faster recovery.
The case of Candida albicans infection, managed successfully with IV fluconazole without surgical intervention, underscores the potential for pathogen-specific, less invasive treatment strategies in select cases. Given these findings, a multimodal approach—incorporating meticulous surgical technique, antimicrobial stewardship, and postoperative wound surveillance—is essential to optimizing outcomes. Additionally, consideration of vascularized flap reconstruction may offer protective benefits in reducing the severity of infectious complications and minimizing the need for repeated debridement.
In two cases where the tumors were considered highly vascularized, preoperative embolization was performed. These patients had a shorter average hospital stay compared to others, and no wound site complications were observed. While it is not yet possible to definitively attribute these favorable outcomes to embolization, the literature highlights several potential benefits [18,19,20]. Embolization reduces intraoperative blood loss, making surgery safer, particularly in large, hypervascular tumors. By blocking the tumor’s feeding arteries, it improves surgical field visibility, minimizes bleeding, and facilitates dissection, which may also contribute to a reduction in surgical duration. Additionally, lower intraoperative blood loss can decrease the need for perioperative blood transfusions and their associated risks. Another important advantage is the enhancement of tumor resectability, as reduced vascularization allows for a more controlled and effective resection [18,19,20].Furthermore, embolization may help lower the risk of postoperative complications such as wound infections and hematoma formation. Although further studies are needed to establish a direct causal relationship, embolization appears to be a valuable adjunct in the surgical management of highly vascular sacral tumors [18,19,20].
Limitations and strengths
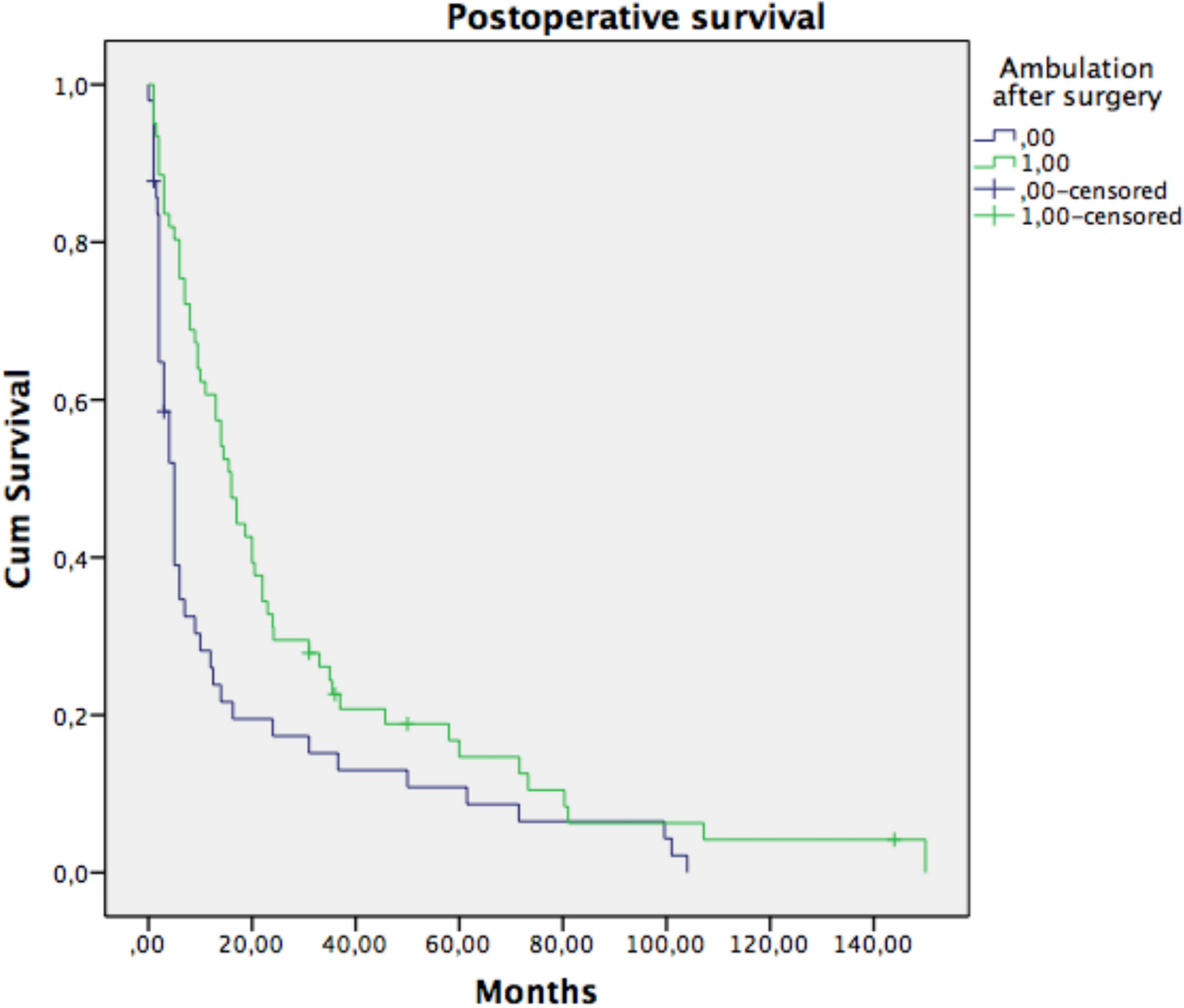
This study has several strengths, particularly its clinical relevance in addressing postoperative infections and complications in oncological sacrectomy, a complex and high-risk surgical procedure. The detailed methodology, including well-defined inclusion and exclusion criteria and a clear description of surgical techniques, enhances the study’s reliability and reproducibility. Additionally, the use of robust statistical tools such as SPSS and Kaplan-Meier survival analysis strengthens the interpretation of the data, providing meaningful insights into patient outcomes. The discussion on polymicrobial infections and the role of reconstructive techniques, such as VRAM flaps, adds significant value by offering practical implications for infection management and wound healing in sacral tumor surgery.
However, some limitations should be acknowledged. The study’s retrospective design inherently limits the ability to establish causal relationships between variables. Additionally, while the sample size provides useful insights, a larger, multicenter cohort would enhance the generalizability of the findings. Another limitation is the lack of standardized infection prevention protocols across cases, which may introduce variability in outcomes. Lastly, the study does not include a direct comparison of embolization versus non-embolization cases, making it difficult to determine the precise impact of embolization on postoperative recovery and complication rates. Future prospective studies with larger patient cohorts and standardized perioperative protocols would further validate the findings and improve clinical applicability.

Comments (0)