
Remember me


The characteristics of the entire study cohort can be found in Supplementary Table 1. The propensity score matched study cohort with their demographic, densitometric, and mechanographic characteristics is presented in Table 1. After propensity score matching there were almost no significant differences in age, weight, height, BMI, and DXA values between the XCT1 and XCT2 cohorts, despite deviations in spinal T-score and CRT time per repetition but with small effect size (Spinal T-score: −1.6 in XCT1 vs. −1.4 in XCT2, p = 0.008, r = 0.09; CRT time per repetition: 1.94 s in XCT1 vs. 2.10 s in XCT2, p = 0.003, r = 0.11). DXA measurements revealed that most of the patients were within the range of osteoporosis (48.5% in XCT1 and 43.5% in XCT2) and osteopenia (42.3% in XCT1 and 47.5% in XCT2). In addition, we detected sarcopenia in 17.0% and 18.8% of the included patients in XCT1 and XCT2, respectively. Bone microstructure characterization with overall values below the range for age- and sex-specific reference values were found in patients with adequate motion grading (Grades 1 to 3) in the propensity score matched cohort (Supplementary Table 2).
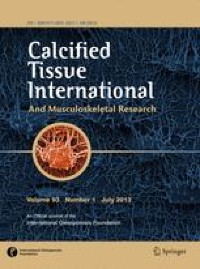
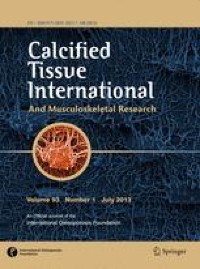
Table 1 Overview of the propensity score matched study cohortComparison of Motion Grading in and Between Both Generations of HR-pQCTAt the distal radius, 35.3% of the scans by XCT1 and 15.5% by XCT2 were graded with 4 to 5 and were therefore inadequate for clinical evaluation (p < 0.001, r = 0.23) (Fig. 2A, B). When comparing motion grading at the distal radius of both device generations, a significantly lower mean motion grading score with medium effect size was found for XCT2 (p < 0.001, r = 0.32) (Fig. 2C). At the distal tibia, 5.3% of the scans by XCT1 and 6.0% by XCT2 were inadequate for clinical evaluation (p = 0.645, r = 0.02) (Fig. 2D, E). When comparing mean motion grading at the distal tibia of both device generations a significantly lower motion grading score with small effect size was found for XCT2 (p = 0.002, r = 0.11) (Fig. 2F). In this context, XCT2 shows more grade 1 scans with 63.8% than XCT1 with 50.3% at the tibial site (p < 0.001, r = 0.14). Furthermore, mean motion gradings were lower at the tibia compared to the radius in both generations of the HR-pQCT (XCT1: 1.7 at the tibia vs. 3.0 at the radius, p < 0.001, r = 0.54; XCT2: 1.6 at the tibia vs. 2.3 at the radius, p < 0.001, r = 0.34).
Fig. 2
Comparison of motion grading distribution for both generations of HR-pQCT in the propensity score matched cohort. Frequency distribution of motion grading at the distal radius (A, B) and tibia (D, E). Comparison of motion grading between the first- and second-generation HR-pQCT at the same site (C, F). Significant differences in the group comparisons are indicated by exact p values with corresponding effect size r
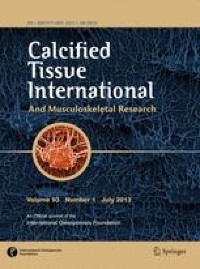
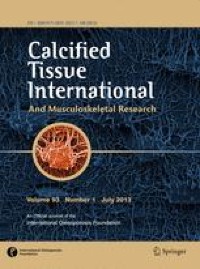
Association of Demographic, Muscle Performance, and Balance Parameters With Motion GradingFor XCT1, significant correlations were found between motion grading at the radius with motion grading at the tibia, sex, age, weight, height, grip strength, and CRT maximum force (Fig. 3A). At the tibia in XCT1, we could show significant correlations between motion grading at the tibia with motion grading at the radius and sex.
Fig. 3
Analyses of motion grading associations in the respective HR-pQCT. Heatmap with correlations of motion grading with the motion grading of the other extremity and demographic, muscle performance, and balance parameters (A). Comparison of motion grading in subgroups based on the clinical cut-off value for motion grading (1–3 ≙ adequate, 4–5 ≙ repetition recommended) at the other extremity (B, C). MG Motion grading; CRT Chair rising test; max. Maximum; rep. Repetition, pleo Path length eyes open; plec Path length eyes closed. Numbers in bold indicate statistical significance (p < 0.05). Significant differences in the group comparisons are indicated by exact p values with corresponding effect size r
For XCT2, significant correlations were found between motion grading at the radius with motion grading at the tibia, age, height, and CRT time per repetition (Fig. 3A). At the tibia in XCT2, significant correlations between motion grading at the tibia with motion grading at the radius and sex, age, weight, height, BMI, grip strength, CRT maximum force, and Romberg path length eyes open were found. While significant correlations between motion grading with the motion grading of the other extremity, female sex, age, CRT time per repetition, and Romberg posturography were positive, significant correlations with weight, height, BMI, grip strength, and CRT maximum force were negative in both device generations. Highest correlations in both device generations were found between the motion gradings of the radius and tibia (XCT1: r = 0.202, p < 0.001; XCT2: r = 0.259, p < 0.001).
Patients were classified into two subgroups based on the clinical motion grading cut-off value (Grades ≤ 3 vs. Grades ≥ 4) for each extremity, respectively. Significantly higher motion gradings at the other extremity were found in patients in the high motion grading group for radius and tibia in XCT1 (Radius: p = 0.007, r = 0.12; Tibia: p = 0.003, r = 0.13) (Fig. 3B) and XCT2 (Radius: p = 0.003, r = 0.13; Tibia: p < 0.001, r = 0.21) (Fig. 3C).
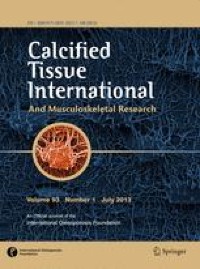
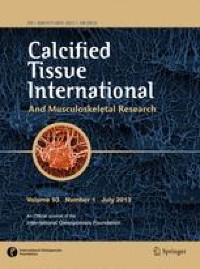
Subgroup-Specific Differences in Motion GradingWe subsequently divided our patients into groups for age, sex, body height, bone mineral density, and sarcopenia. For this purpose, we chose the following group distributions: sex according to male and female, age according to < 50 years old, 50–69 years old, and ≥ 70 years old, height according to < 1.60 m, 1.60 m to 1.79 m, and ≥ 1.80 m, bone mineral density according to T-score classified into normal BMD (≥ −1.0), osteopenia (< −1.0 to −2.4), and osteoporosis (≤ −2.5), and muscle performance classified into normal muscle performance and sarcopenia using thresholds based on grip strength and CRT time per repetition, as recommended by the EWGSOP2 consensus [16] (Fig. 4).
Fig. 4
Motion grading in clinical subgroups in both generations of HR-pQCT. Comparison of clinical subgroups regarding motion grading in first- and second-generation HR-pQCT at the distal radius (A, C) and tibia (B, D). Significant differences in the group comparisons are indicated by exact p-values with corresponding effect size r
At the radius in XCT1, significant differences could be found when comparing sex and age (all p ≤ 0.001, r = 0.18 to 0.28) with a higher mean motion grading in the female group (Fig. 4A). There were no significant differences present in the groups of height, BMD, and sarcopenia. At the tibia, in XCT1 a significant alteration only in motion grading between the sexes (p = 0.019, r = 0.11) (Fig. 4B) was detected with a higher mean motion grading in women.
In XCT2 at the radius, significant differences could be shown between the groups in age and height (all p < 0.05, r = 0.19 to 0.23), but not in sex, BMD, and sarcopenia (Fig. 4C). At the tibia, in XCT2 significant differences were measured in motion grading between the groups in sex, age, height, and BMD (all p < 0.05, r = 0.13 to 0.29) (Fig. 4D).
Taken together, women and older patients exhibit higher mean motion grading and no differences in motion grading could be detected between the groups with normal muscle performance compared to sarcopenia. In XCT2, additionally, shorter patients tend to exhibit significantly higher motion artifacts. Also, patients with lower bone mineral density tend to show significantly higher motion gradings in the tibial XCT2 scans only.
Identifying Independent Predictors of Motion GradingWe applied a multiple linear regression model to identify independent predictors of motion grading at the distal radius and tibia for both device generations (Table 2). Therefore, we included the parameters which showed the strongest correlations in our previous analyses. Among these belong sex, age, height, and the motion grading of the other extremity. In total, all multiple linear regression models were significant (p < 0.001) and the adjusted R2 ranged from 0.039 to 0.105. The motion grading of one extremity proved to be an independent predictor of the motion grading of the other extremity in all cases. Age could also be identified as an independent predictor of the motion grading, but only for the radius in XCT1 and the tibia in XCT2. Moreover, body height could be shown to independently predict the motion grading of the tibia in XCT2, while sex was not an independent predictor of motion grading in any of the sites or device generations.
Table 2 Results of multiple linear regression models analyzing independent factors associated with motion grading at the distal radius and tibia in HR-pQCT on both device generations
Comments (0)