
Remember me

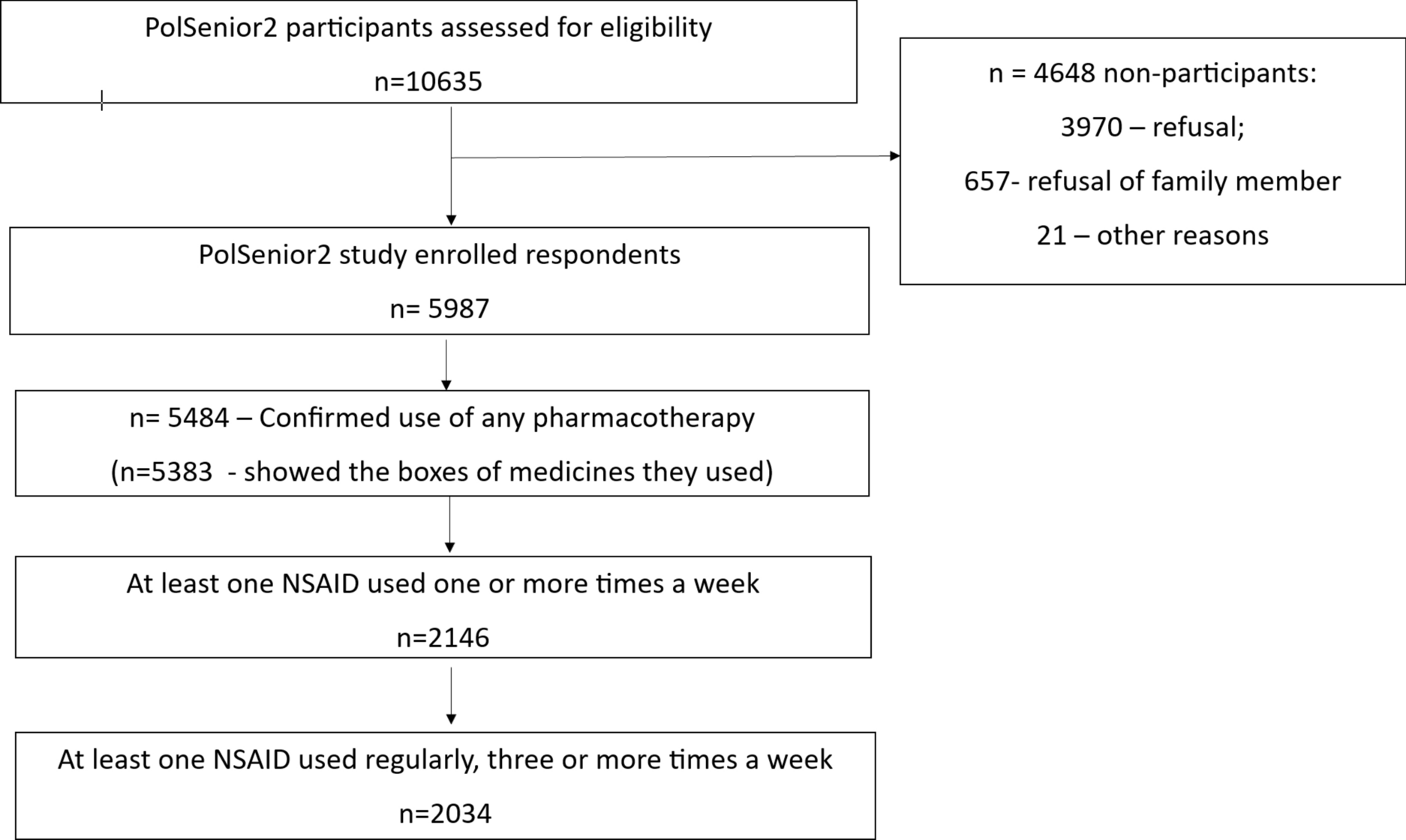
A PRISMA flow diagram of the study selection process is shown in Fig. 1. A total of 39 studies were included after inclusion and exclusion criteria were applied.
Fig. 1
Preferred reporting items for systematic reviews and meta-analyses flow diagram
The study characteristics, key findings, and risk of bias are summarized in Table 1.
Table 1 Study characteristics and bias rating (n = 39)The sample size varied from 173 to 1,169,894, with a total sample size of 1,338,737 people living with dementia in the community. Of the studies, 17 included various analyses from a single population cohort, the Finnish Medication and Alzheimer’s disease (MEDALZ) study database [24]. The MEDALZ study population was only counted once in the total subject sample of this review. However, each MEDALZ study cohort paper investigated a different outcome within this cohort and was included individually in the synthesis. Three large US studies based on Medicare administrative data were included; however, the population numbers were only included once to minimize the risk of over-inflation.
The country of origin of the studies included Finland (n = 18), the USA (n = 11), Canada (n = 3), Germany (n = 2), Italy (n = 1), Norway (n = 1), Sweden (n = 1), the Netherlands (n = 1), and France (n = 1). The participants’ ages ranged from 37 to 100 years. One study specifically focused on people with younger onset dementia (ages < 65 years) [25], and one specifically on males [26].
The majority (n = 26; 67%) of the studies were rated as having a low risk of bias and corresponding good quality, and 13 (33%) studies were rated as having a moderate risk and fair quality. None were rated as having a high risk of bias or low quality. Agreement between independent assessors was high, with 90% agreement across the studies. All studies used quantitative or mixed methodologies. Five were prospective cohort studies, 29 were retrospective cohort studies, four were cross-sectional studies, and one was a nested case-control study.
4.2 Thematic Analysis and SynthesisFollowing an inductive process and thematic analysis, factors common to the use of all psychotropic medications and factors associated with using specific classes of psychotropic medications were identified.
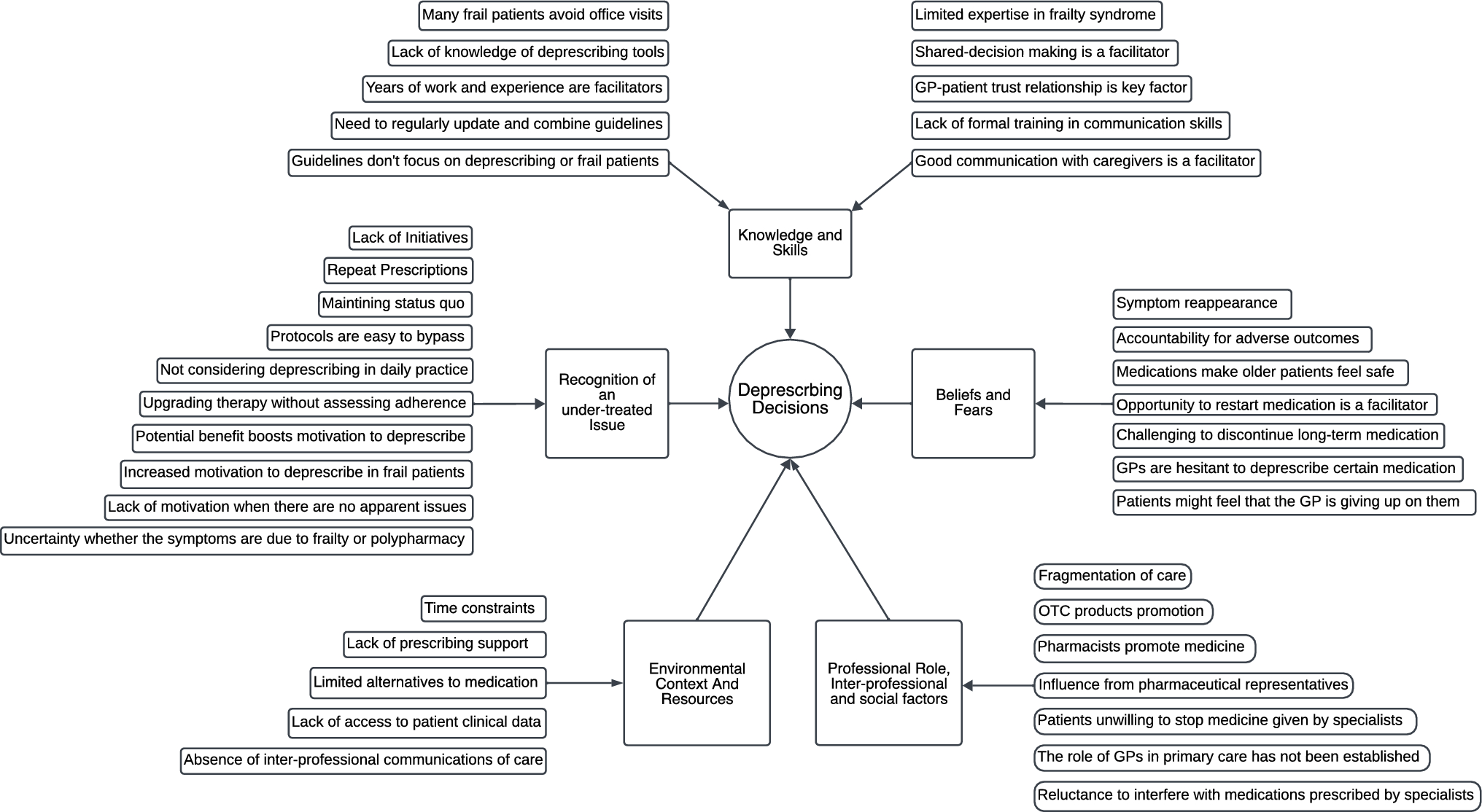
The thematic trends that emerged from the analysis are summarized for both psychotropic medications in general and the different classes of psychotropic medications in Fig. 2. When combined, these general and class-specific factors were grouped into higher-order themes: (1) patient related, (2) illness related, (3) environmental, (4) carer related, and (5) prescriber related or prescribing trends. Thematic analysis did not identify differences in outcome themes when studies were grouped according to type (retrospective/prospective longitudinal cohort or cross-sectional).
Fig. 2
Summary of identified themes
4.2.1 Theme 1: Patient-Related Factors4.2.1.1 SexWomen were more commonly prescribed antidepressants, anxiolytics/hypnotics, and opioids than men, who received more antipsychotic and anticonvulsant medications. Six of the seven papers reporting on anxiolytic/hypnotic medications and sex found a significantly greater percentage of females prescribed anxiolytics/hypnotics than males [8, 27,28,29,30,31]. The majority of these papers (5/6) were retrospective longitudinal cohort studies of good quality and low risk of bias. One paper [25], a prospective longitudinal cohort study of good quality and low risk of bias, found no sex difference in their population of young onset people with dementia. Of the four papers that reported the use of opioids, all identified a significant difference in favor of females [8, 27, 28, 32]. Three out of the four studies were rated as good quality and low risk of bias. Eight of the ten papers that reported sex and antidepressant use found greater female use of antidepressants [8, 27, 30, 33,34,35,36,37]. Seven of these were longitudinal cohort studies (six retrospective and one prospective) and one was a cross-sectional analysis of a prospective cohort). Five of the eight studies were good quality and low risk of bias. The two remaining papers found no difference between males and females [25, 38]. Of these two papers, one represented a unique younger onset dementia population [25], while the other investigated carer and care recipient factors rather than sex, which may have influenced the outcomes of this finding [38]. Both were of good quality and low risk of bias. One was a prospective longitudinal cohort, the other was a cross-sectional analysis of a retrospective cohort. Antipsychotics were utilized more frequently in males compared with females in six papers [27, 36, 39,40,41,42]. Of these two were retrospective cross-sectional analyses, two were prospective longitudinal cohorts, and two were retrospective longitudinal cohorts. Two papers, both retrospective longitudinal cohorts, reported greater use in females [8, 43] and one, a retrospective longitudinal cohort, identified that females were prescribed antipsychotics more commonly prior to diagnosis compared with males [44]. The use of anticonvulsant drugs was reported in one study, where males used anticonvulsants significantly more than females (p < 0.001) [45].
4.2.1.2 EthnicityThere was sparse data relating to ethnicity. One paper [46] investigated this as the primary objective, identifying that anxiolytic use was more common in African American people with dementia, while antipsychotics were used more frequently in non-Hispanic white people. No consistent trend was identified in the other available papers reporting on ethnicity as secondary outcomes [8, 38, 42].
4.2.1.3 AgeThere were 20 papers available for synthesizing age and psychotropic use. There was increased use of psychotropics in older individuals (> 80 years) before dementia diagnosis and increased association with psychotropic use in younger individuals (< 75 years) immediately following diagnosis [9, 28, 44]. All three of these studies were of good quality and low risk of bias. A second trend was identified for “very old” people (defined in the paper as > 90 years) in whom the use of psychotropics appeared to be higher than those < 90 years old [47]. Younger individuals (< 75 years) received more antidepressant, antipsychotic, and anticonvulsant medications [8, 37, 42, 48], while older individuals were prescribed more benzodiazepines and opioids [27, 28, 32, 49]. There was a consistent trend for younger individuals to have more psychotropic polypharmacy [9, 50, 51]. These findings were consistent across both the longitudinal and cross-sectional studies.
4.2.1.4 Psychiatric ComorbidityThe use of psychotropic polypharmacy was significantly associated with having a psychiatric history in four papers [9, 28, 50, 51]. Although there was no significant association between a history of mental disorders and antipsychotic use in Eichler et al.’s study, sample numbers were low, with only 140 participants included in the factor analysis, of whom 22 were on antipsychotic medication [52].
A history of depression and antidepressant use was associated with increased use of antipsychotics [9, 40, 41, 44, 50, 51, 53, 54]. The use of benzodiazepines and/or opioids was significantly associated with a history of prior substance abuse [28, 29, 32].
Highly significant associations with prior diagnoses of psychiatric illness (schizophrenia, bipolar disorder, or depression) were also demonstrated for long-term benzodiazepine use (p < 0.0001) [31] and high-dose antipsychotic use (p < 0.0001) [55]. Anticonvulsant use was also significantly associated with depression, schizophrenia, and bipolar disorders (p < 0.001 for all), although only formally investigated in one study [45].
4.2.1.5 PainOnly two studies specifically investigated pain in relation to psychotropic use. Grace et al. [38] reported a significant association between pain and antipsychotic use. Hamina et al. [56] identified that opioid initiation triggered an immediate increase in benzodiazepine and antipsychotic use, with a nonsignificant decrease in the use of these agents up to 6 months post-opioid initiation.
4.2.2 Theme 2: Illness-Related Factors4.2.2.1 Severity of DementiaAntipsychotic use did not increase in parallel with the severity of cognitive impairment. Antipsychotic use was significantly associated with moderately severe dementia (as opposed to mild or severe) in all three papers that reported on this [48, 52, 57]. One paper found no association between cognition (measured by the Mini-Mental State Examination) and antipsychotic use; however, Mini-Mental State Examination scores were not categorized as mild, moderate, or severe, and a cumulative value was used, which may have influenced the findings [58]. Two papers reported a significant association between antipsychotic use and greater severity on the Clinical Dementia Rating sum of boxes scale [42, 58]. No trend was identified between cognitive functioning and other classes of psychotropics. All the papers above were rated as moderate risk of bias apart from one [48], which was rated a low risk of bias. Three of the studies were cross-sectional in nature [42, 48, 52] and two were longitudinal cohorts of up to 1 year follow-up [57,
Comments (0)