2.1 Study Design and Setting
This study was reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines (http://www.strobe-statement.org). A completed STROBE checklist is provided as Supplementary Material 3 (see electronic supplementary material [ESM]).
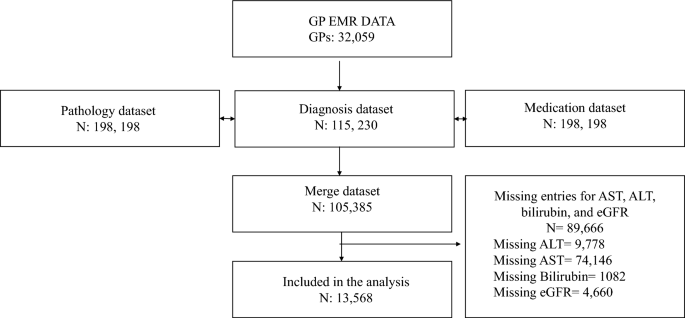
We conducted a cross-sectional study (data analysed from January 2013 to December 2022) using electronic data from general practitioners (GPs) across Australia. Data were obtained from the IQVIA ‘general practice electronic medical record’ (GP EMR) database, which contains de-identified in-patient records across the Australian primary care setting. IQVIA is a health data analytics company that provides de-identified patient records used for research and quality purposes. The GP EMR dataset represents approximately 12% of Australian primary care practices, based on national GP workforce data. Ethical approval for this study was obtained from the Monash University Human Research Ethics Committee (MUHREC project ID: 44395).
2.2 Participants and Data
The study population consisted of people aged 18 years and older, who were prescribed at least one LLT based on the Anatomical Therapeutic Chemical Classification System (ATC) ‘C10’ code [18]. Diagnoses were clinician-entered and mapped to ICD-10-AM codes using standardised algorithms of the International Classification of Diseases Australian Modification, 10th revision (ICD-10-AM) using standardised coding algorithms.
Variables included demographic data (age, sex, smoking status), clinical diagnoses (hypertension, hyperlipidaemia, CKD, diabetes), and medication classes (antithrombotics, antihypertensives, LLTs, smoking cessation therapies). Pathology data included biomarkers such as alanine transaminase (ALT), aspartate transaminase (AST), and bilirubin, for testing of liver function, and estimated glomerular filtration rate (eGFR) for testing of kidney function. Biomarker values were extracted from routine pathology records linked to the EMR. Patients missing any of the key biomarkers (ALT, AST, bilirubin, or eGFR) were excluded from the analysis.
2.3 Exposure
Polypharmacy was examined both as an exposure and as an outcome in this study. First, CVD-related polypharmacy was treated as an outcome to identify demographic and clinical predictors associated with its prevalence, using multivariable logistic regression. Second, polypharmacy was also analysed as an exposure to assess its association with liver and kidney dysfunction.
CVD-related polypharmacy was defined as the concurrent use of five or more CVD-related prescription medications including LLT, antithrombotics, antihypertensives, and other cardiovascular therapies, within a 365-day sliding window between 2013 and 2022. The sliding window approach allowed for periodic recalculation of medication counts by shifting the start and end dates, thereby capturing temporal variation in prescribing and better reflecting real-world medication exposure. To account for medication substitutions within the same therapeutic class, medication types were defined using the first four digits of the Anatomical Therapeutic Chemical (ATC) classification code. This approach ensured that medications within the same therapeutic class were not counted multiple times and enabled the calculation of medication class counts. A sensitivity analysis was conducted using shorter sliding windows of 90 and 180 days to test the robustness of the polypharmacy definition (Supplementary Material 1, ESM). A list of the CVD-related medications including medication classes is provided in Supplementary Material 2 (ESM). The analysis was restricted to CVD-related prescriptions available within the dataset.
2.4 Outcomes
The main outcomes were CVD-related polypharmacy described in the previous section and the prevalence of liver and kidney dysfunction. Kidney and liver function were assessed using median values across all available biomarker measurements to reduce the influence of outliers and reflect typical levels over time [19,20,21,22]. Kidney function was evaluated using eGFR [23]. Kidney dysfunction was defined as eGFR <90 mL/min/1.73 m2. Liver function was assessed using bilirubin, alanine transaminase (ALT), or aspartate transaminase (AST). Reference ranges were defined as bilirubin 1–20 µmol/L, ALT 5–40 U/L for males and 5–35 U/L for females, and AST 5–35 U/L for males and 5–30 U/L for females. Biomarker values were extracted from routine pathology records recorded between 2013 and 2022. Where multiple measurements were available, patient-level median biomarker values were calculated across the observation period to summarise typical liver and kidney function and minimise the influence of extreme values. Detailed reference thresholds and classification criteria are provided in Supplementary Material 2 (ESM).
2.5 Statistical Analyses
Descriptive statistics were used to characterise the study population. Continuous variables were summarised as medians with interquartile ranges (IQR) for non-normally distributed data. Categorical variables were presented as frequencies and percentages. Normality of continuous variables was assessed using the Kolmogorov Smirnov test in conjunction with visual inspection of histograms and Q to Q plots. For between-group comparisons, we utilised Student’s t-test for normally distributed continuous variables and the Mann–Whitney U test for non-normally distributed continuous variables. For categorical variables, the chi-square test was applied. Pearson’s chi square test was used to compare categorical variables.
Six logistic regression models were constructed. Models 1 and 2 examined predictors of CVD-related polypharmacy, with polypharmacy defined as the outcome variable. Model 1 included age and sex. Model 2 additionally adjusted for hyperlipidaemia, hypertension, diabetes, and smoking status.
Models 3 and 4 assessed the association between polypharmacy and kidney dysfunction, with kidney dysfunction defined as the outcome variable and polypharmacy as the primary exposure. Model 3 adjusted for age and sex, while Model 4 additionally adjusted for hyperlipidaemia, hypertension, diabetes, and smoking status.
Models 5 and 6 evaluated the association between polypharmacy and liver dysfunction, with liver dysfunction defined as the outcome variable and polypharmacy as the primary exposure. Model 5 included age and sex, and Model 6 additionally adjusted for hyperlipidaemia, hypertension, diabetes, and smoking status.
Covariates were selected based on clinical relevance and established associations with cardiovascular disease and medication burden. Multicollinearity was assessed using variance inflation factors, with no evidence of problematic collinearity identified. Adjusted and unadjusted odds ratios (ORs) with 95 percent confidence intervals (CIs) were reported. Statistical significance was defined as a two-sided p-value <0.05.
Given the use of a large national electronic medical record dataset, all eligible patients meeting inclusion criteria during the study period were included and no formal sample size calculation was performed. Sensitivity analyses were conducted using alternative polypharmacy definitions based on 90-day and 180-day sliding windows to assess the robustness of the findings.
Sensitivity analyses were conducted to evaluate the utility of the ALT/AST ratio in identifying hepatocellular damage and its association with polypharmacy. Receiver operating characteristic (ROC) curve analyses were performed to compare the discriminatory performance of the ALT/AST ratio with individual biomarkers (ALT, AST, and total bilirubin), with full details provided in Supplementary Material 4 (ESM).
All statistical analyses were performed using Stata version 14.1 (StataCorp, College Station, Texas, USA).
To explore associations, six logistic regression models were constructed:
Model I (crude polypharmacy): Polypharmacy as the outcome, with age and sex as predictors.
Model II (adjusted polypharmacy): Polypharmacy as the outcome, with age, sex, hyperlipidaemia, hypertension, diabetes, and smoking status as predictors.
Model III (crude kidney): Kidney dysfunction as the outcome, with polypharmacy as the primary exposure and adjustment for age and sex.
Model IV (adjusted kidney): Kidney dysfunction as the outcome, with polypharmacy as the primary exposure and additional adjustment for age, sex, hyperlipidaemia, hypertension, diabetes, and smoking status.
Model V (crude liver): Liver dysfunction as the outcome, with polypharmacy as the primary exposure and adjustment for age and sex.
Model VI (adjusted liver): Liver dysfunction as the outcome, with polypharmacy as the primary exposure and additional adjustment for age, sex, hyperlipidaemia, hypertension, diabetes, and smoking status.



Comments (0)