
Remember me


Mandibular osteoid osteoma is distinctly uncommon and may become particularly challenging to manage after prior surgical intervention [1]. We report the case of a 25-year-old woman with histopathologically confirmed recurrent osteoid osteoma of the left mandibular corpus and persistent severe nocturnal pain despite three prior surgical resections since 2021. At presentation, pain was rated 9/10 without analgesics and 3/10 while receiving tilidine. The patient additionally described progressive displacement of the adjacent tooth. Repeat segmental mandibular resection was considered disproportionately invasive in view of recurrent disease, postsurgical distortion of the mandibular anatomy, and the close proximity of the lesion to the mental foramen and inferior alveolar nerve. A minimally invasive image-guided salvage strategy was therefore pursued (Fig. 1).
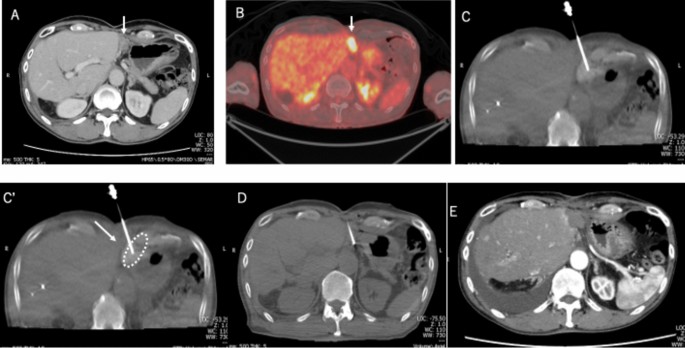
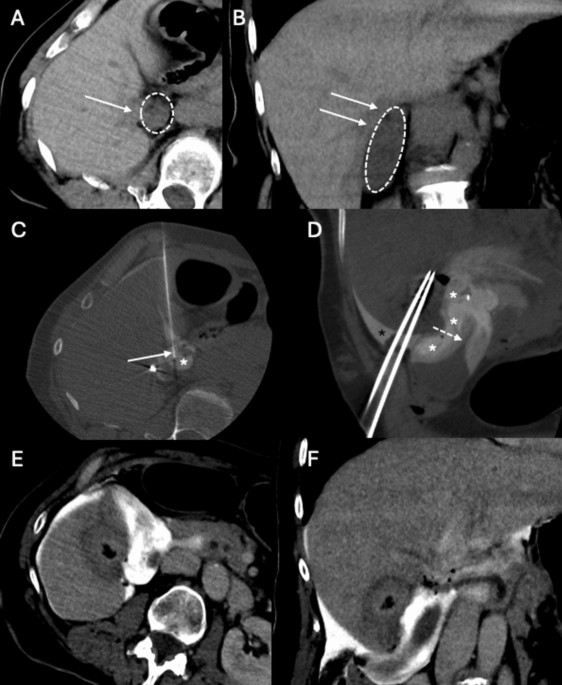
Fig. 1 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.CT-guided transmandibular cryoablation of recurrent mandibular osteoid osteoma. A Planning CT shows the nidus (blue arrow) adjacent to the inferior alveolar nerve region (red arrow). B After transmandibular drilling, the cryoprobe is positioned centrally within the nidus. C Postprocedural CT shows the drill tract (blue arrow) with preserved osseous boundaries of the inferior alveolar nerve canal (red arrow)
The procedure was performed under general anesthesia with CT guidance. Intraprocedural imaging localized the residual nidus within the medial mandibular cortex. Because prior resections had substantially altered the lateral cortical anatomy, a conventional lateral access route was not feasible. A transmandibular osseous corridor through the mandibular body was therefore established. A powered triaxial bone access system was advanced through the cortex to the target, permitting mechanical disruption of the sclerotic tissue. Subsequently, a 17G cryoprobe was positioned centrally within the nidus, and a single 6-min freeze cycle was applied.
Cryoablation was favored over hyperthermic ablation because the lesion was situated in a surgically altered, high-risk craniofacial region adjacent to the inferior alveolar nerve and mental foramen. In this setting, cryoablation was considered advantageous because cold-based ablation is generally associated with superior preservation of collagenous and neural structures compared with heat-based techniques, while still allowing CT-guided control of the treatment geometry [1,2,3]. Although the intramedullary extent of the ice ball cannot be fully visualized within cortical bone, procedural safety was supported by meticulous CT-based trajectory planning and by maintaining an approximately 2 mm distance between the cryoprobe tip and the inferior alveolar nerve. During cortical passage, the drill sleeve additionally served as a mechanical shield for the mental nerve. A single rather than double freeze cycle was deliberately selected because the cryoprobe could be positioned centrally within the nidus, rendering one cycle sufficient while minimizing the theoretical risk of neural injury.
The procedure was completed without immediate major complications. On the first postprocedural day, the patient reported complete pain relief with a visual analog scale score of 0/10. A mild transient tension-type headache occurred. Sensory numbness in the affected region had already been present at baseline and did not worsen clinically after the intervention; no motor deficit was observed. The patient was discharged the following day without an analgesic requirement. At 1-week follow-up, pain relief remained complete and the sensory symptoms had improved.
This case demonstrates that CT-guided cryoablation can be successfully adapted to recurrent mandibular osteoid osteoma even in complex postsurgical anatomy. While radiofrequency ablation remains the best established minimally invasive treatment for osteoid osteoma [1, 4], cryoablation offers particular advantages in anatomically constrained regions by enabling controlled treatment adjacent to vulnerable structures and has shown excellent technical and clinical efficacy in published series [2, 3]. In the present case, the decisive technical modification was the transmandibular approach, which created a controlled osseous access route when standard lateral access was no longer possible after repeated resections. Previous reports on cryoablation of benign mandibular bony lesions further support the feasibility of carefully planned cold-based intervention in this region [1].
Radiation exposure likewise warrants contextualization. In the present case, the cumulative CTDIvol was 25.86 mGy and the DLP was 87 mGy·cm. Compared with contemporary registry data on conventional CT-guided osteoid osteoma ablation, this exposure appears low and remains within the lower reported range [5]. Nevertheless, conventional CT was considered preferable in this craniofacial setting because it enabled precise trajectory planning and confident monitoring in close proximity to the inferior alveolar canal and mental foramen.
In conclusion, CT-guided transmandibular cryoablation appears to be a feasible, safe, and effective salvage treatment option for recurrent mandibular osteoid osteoma after multiple surgical resections. Careful trajectory planning, central probe placement, maintenance of a small CT-confirmed distance to the inferior alveolar nerve, and dedicated nerve protection measures enabled successful treatment without new motor neurological sequelae. This technique may broaden the role of percutaneous ablation in selected craniofacial lesions that would otherwise require more extensive reoperation.
Comments (0)