As OA prevalence accelerates, more THA and TKA procedures will inevitably yield more revisions, amplifying patient morbidity and health system costs [29]. Optimization of peri-implant bone metabolism through antiresorptive therapy represents a biologically plausible strategy that may be associated with improved implant durability, although causal effects cannot be inferred from observational data. Against this background, we investigated the association between perioperative antiresorptive therapy with denosumab versus alendronate and the cumulative incidence of revision after primary THA and TKA for OA.
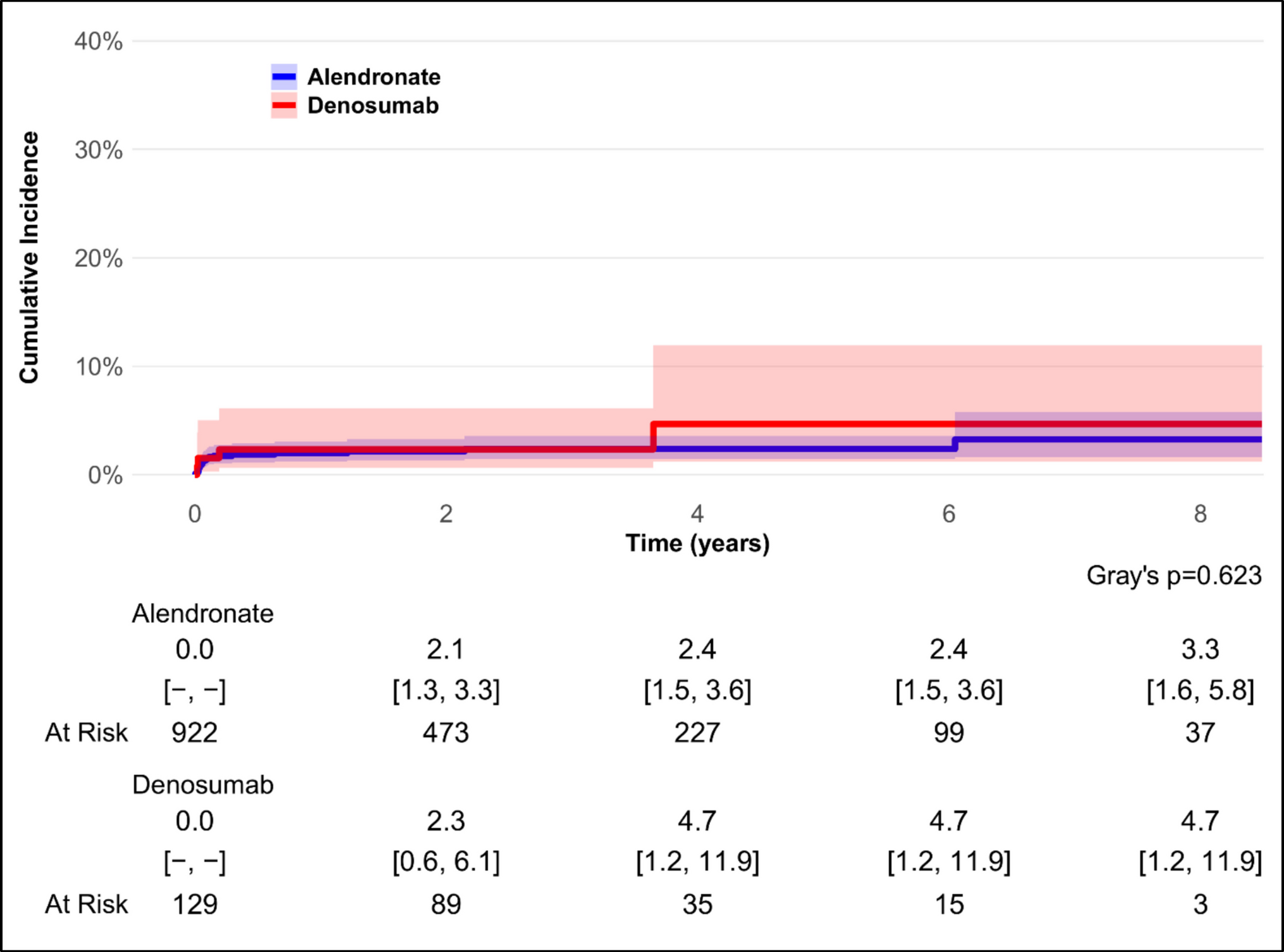
In the THA cohort, the cumulative incidence of revision remained low and comparable between treatments, with no between-group differences. This is consistent with randomized evidence showing that denosumab preserves periprosthetic BMD after uncemented THA but does not measurably improve early mechanical fixation. In a double-blind randomized trial of postmenopausal women, denosumab administered one month before surgery and again at 6 months significantly attenuated calcar bone loss in Gruen zone 7 and increased BMD in the trochanteric regions, yet did not reduce femoral stem subsidence or rotations assessed by radiostereometric analysis (RSA) up to 48 weeks [23]. All stems achieved osseointegration, and functional recovery was comparable between arms [23]. In another randomized placebo-controlled study, denosumab given 1–3 days after THA and repeated at 6 months prevented early periprosthetic bone loss, producing marked BMD gains at 12 months (approximately + 32% in Gruen 7 and + 11% across zones 1–7), though this effect waned after discontinuation and was not accompanied by any difference in clinical outcomes [30]. Similarly, in a head-to-head randomized comparison, denosumab outperformed risedronate in maintaining proximal femoral BMD through 24 months, particularly in Gruen zones 1 and 7, while no data on implant migration or revision were collected [22].
In the TKA cohort, the cumulative incidence of revision differed markedly between treatment groups, with a higher revision incidence observed among denosumab users. The imbalance was mainly driven by aseptic tibial component loosening, whereas only a single revision was related to infection. This pattern was further supported by exploratory competing risk analyses focusing specifically on aseptic loosening, which showed no significant difference between treatments in THA but confirmed a higher cumulative incidence of loosening among denosumab users in TKA. A plausible explanation may lie in the interaction between denosumab’s reversible antiresorptive effect and the intense mechanical stresses acting on the tibial interface [31]. In this setting, any transient alteration in bone turnover could theoretically hinder the continuous remodeling required to maintain stable osseointegration under load. The tibial component, exposed to high axial and shear forces, represents a structurally more fragile element and may thus be particularly sensitive to any disturbance in bone turnover dynamics [32]. However, the observational design does not allow causal attribution.
These observations appear to diverge from earlier reports suggesting favorable short-term effects of denosumab on tibial fixation and periprosthetic bone quality. In a randomized trial, Ledin et al. reported that two 60 mg injections of denosumab (day 1 and 6 months) reduced early tibial component migration by approximately one-third, as measured by RSA [33]. Likewise, Murahashi et al. found that postoperative denosumab therapy, combined with vitamin D, prevented BMD loss in the proximal tibia after 12 months (+ 0.7% vs − 19.7% in controls) [34]. However, these trials were small, short in duration, and focused on surrogate imaging endpoints rather than clinical revision.
In contrast, our registry-based study evaluated the cumulative incidence of revision surgery as a hard clinical outcome over longer follow-up. The comparison with an active antiresorptive therapy such as alendronate should also be considered when interpreting these findings. Bisphosphonates have consistently demonstrated benefits on implant fixation and survival after arthroplasty, and the long-term skeletal binding of alendronate may provide more durable antiresorptive conditions than the reversible mechanism of denosumab [13, 18].
Denosumab has been associated with a modest increase in serious infections in meta-analyses of randomized trials [35]. In our cohort, we did not observe an apparent signal of increased infection-related revision among denosumab users, although the limited number of events precludes definitive safety conclusions. Across both hip and knee arthroplasties, only one case of revision for infectious causes was recorded in patients treated with denosumab—a septic loosening following TKA—while no infection-related revisions occurred in the THA group. This finding provides an additional element of safety reassurance, suggesting that the higher revision rate observed among denosumab users was predominantly mechanical rather than infectious in nature. To better understand this pattern, it is essential to consider the pathophysiological basis of aseptic loosening and how antiresorptive therapies may interact with periprosthetic bone remodeling under mechanical stress. Aseptic loosening is driven by inflammatory osteolysis, often triggered by wear debris. These particles activate macrophages, which release pro-inflammatory cytokines and promote RANKL expression, thereby stimulating osteoclastogenesis and periprosthetic bone resorption [36]. This remodeling process is essential not only to clear damaged or necrotic bone but also to allow new bone formation and osseointegration under load [37].
Bisphosphonates, such as alendronate, integrate into the bone matrix and are released locally during bone turnover, exerting a spatially confined and sustained antiresorptive effect [38]. This may permit a balance between reduced resorption and preserved remodeling, allowing controlled adaptation of bone to mechanical stimuli [38]. Indeed, clinical studies have shown that bisphosphonates reduce early migration and improve implant fixation in TKA [39].
Denosumab, by contrast, acts systemically by inhibiting circulating RANKL and causing near-complete suppression of osteoclast activity throughout the skeleton [40]. While effective in increasing BMD and reducing bone turnover markers within weeks, this potent effect may also impair physiological remodeling where it is most needed—at the prosthesis–bone interface [40]. In the tibial metaphysis, where the component rests on a thin layer of cancellous bone with limited cortical support, early remodeling is critical to adapt to high shear and compressive loads [41]. Excessive suppression of resorption could theoretically delay removal of necrotic bone or impede formation of micro-callus, potentially predisposing to micromotion and instability [42]. Moreover, denosumab’s reversibility poses an additional challenge. Upon discontinuation or delayed dosing, there is a documented rebound increase in bone resorption markers and rapid BMD loss [15]. Although our design accounted for adherence, even transient fluctuations in bone turnover may impact long-term integration under stress. Current guidelines for perioperative medication management do not address denosumab, bisphosphonates, or other drugs used in osteoporosis management. Further investigation is needed to better understand the effects of these medications on arthroplasty loosening, including the potential role of administering bisphosphonates prior to TKA in patients receiving other antiresorptive or anabolic agents.
Another relevant consideration concerns patient characteristics. Although baseline demographics were similar, in Italy denosumab is often prescribed to individuals with more severe osteoporosis or contraindications to bisphosphonates, such as renal impairment or significant upper gastrointestinal disease. This may have selected patients with inherently more fragile bone and a predisposition to early mobilization. However, if confounding by indication were the sole explanation, similar differences would be expected in the hip cohort, yet these were not observed. It is therefore plausible that biological and biomechanical factors acted synergistically to amplify the effect in the knee. Further studies should include additional bone measures to clarify the baseline pre-arthroplasty status.
Additional limitations must be considered. This study was designed to estimate associations between perioperative antiresorptive exposure and implant revision using a registry-based framework; results should therefore be interpreted as hypothesis-generating and the observational nature precludes causal inference. The definition of perioperative exposure also deserves consideration. We adopted a ± 180-day window centered on the index arthroplasty to capture pharmacologically relevant antiresorptive exposure during the early peri-implant remodeling phase. Alternative definitions of time zero could address different research questions, such as treatment initiation or longer-term exposure patterns, and might yield different estimates. Treatment allocation was not randomized and unmeasured confounders may persist. We lack direct measures of BMD, FRAX score or other frailty markers. Although exploratory competing risk regression models were performed to adjust for age, sex, and treatment initiation timing, the limited number of events—particularly in the denosumab THA group—restricts the robustness of multivariable modelling. Finally, the analysis is based on an Italian regional population; surgical and prescribing practices may vary in other healthcare systems, and generalisability requires caution.
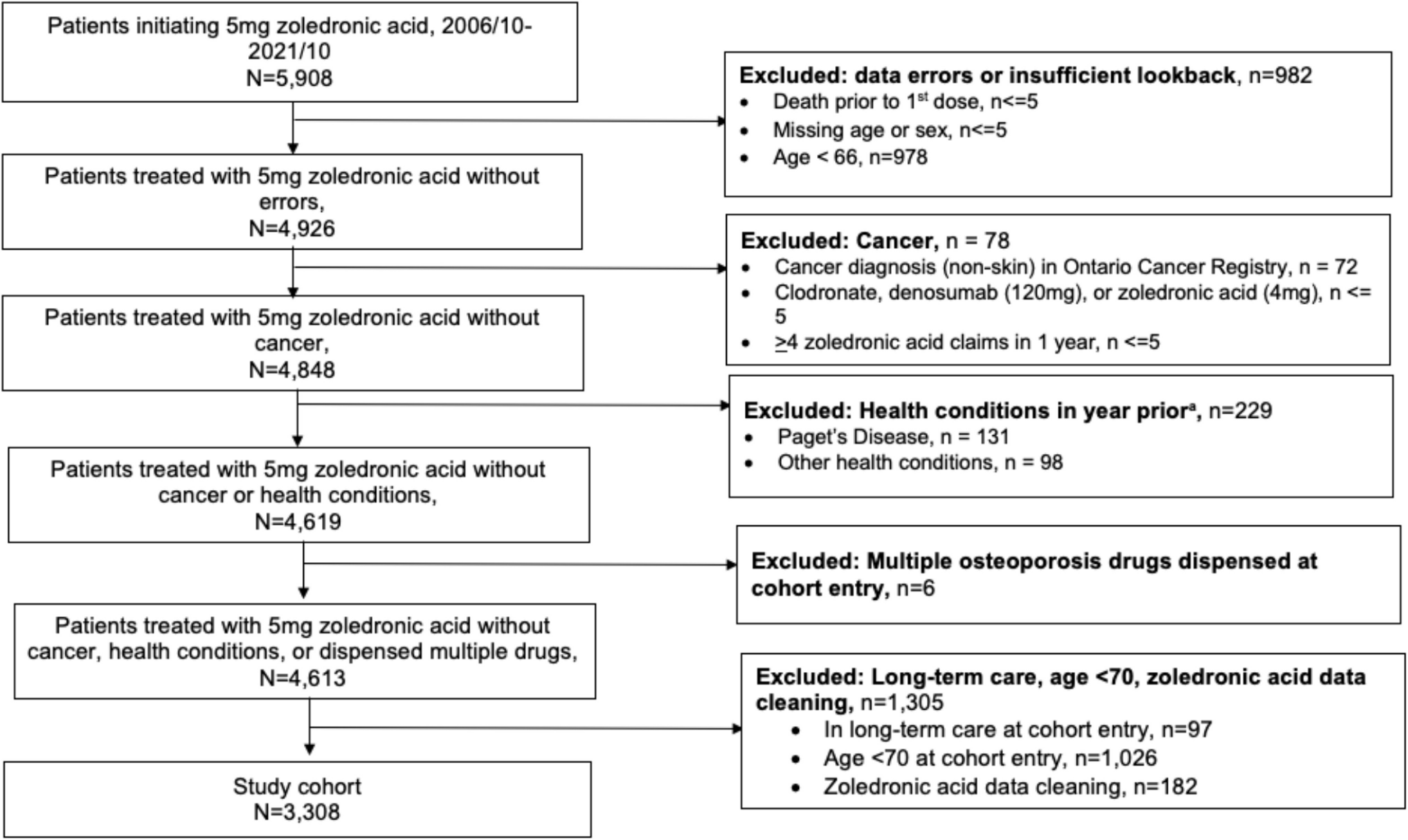
However, our work also has strengths. First, it uses the regional RIPO registry, which records more than 95% of arthroplasties performed in the Emilia-Romagna region and allows almost complete follow-up through linkage with hospital and pharmacy databases. Second, we defined drug exposure rigorously using prescription archives and introduced continuity criteria, limiting the risk of misclassification. Third, the separate analysis of THA and TKA allowed us to highlight joint-specific differences, avoiding the dilution effect that would have resulted from a combined analysis. Fourth, we excluded patients who underwent arthroplasty following acute or prior fracture, because these procedures represent a substantially different clinical scenario compared with elective arthroplasty for OA.
Our results may have practical implications for the perioperative management of OA patients undergoing TKA or THA. In TKA, the association between denosumab and a higher revision risk suggests that alendronate remains a more prudent choice for perioperative osteoporosis management. This observation does not necessarily imply that denosumab is harmful—the absolute difference in revisions is small and the drug has shown important benefits in preventing vertebral and hip fractures—but indicates the need for individualised assessment, considering the patient’s risk profile and the surgical site. Moreover, usual precautions pertaining to rebound bone resorption would preclude denosumab discontinuation prior to TKA [15]. In THA, the substantial equivalence between denosumab and alendronate provides reassurance that therapy can be guided by other clinical considerations, such as tolerability and adherence. Monitoring bone health with DXA remains essential, and preoperative screening in high-risk patients—along with appropriate optimisation of osteoporosis therapy—is strongly recommended [43]. Early identification of osteopenia and osteoporosis may allow timely initiation of treatment before surgery, potentially supporting postoperative recovery and implant stability [44].
In this context, perioperative bisphosphonate use has been associated with improved arthroplasty outcomes and lower revision risk in several large observational studies, supporting the concept that optimizing periprosthetic bone metabolism may enhance implant durability [16, 19, 20]. However, real-world evidence remains heterogeneous, and some recent database analyses focusing on preoperative exposure have not demonstrated clear benefit and, in selected populations, have reported higher early complication rates [45, 46]. These findings suggest that perioperative antiresorptive strategies should be individualized and guided by fracture-risk assessment, while optimal timing and patient selection remain priorities.
The differences found in our study suggest various lines of future research. Prospective controlled studies are needed to directly assess the effectiveness of denosumab versus bisphosphonates in terms of implant survival, including detailed measures of BMD, tibial trabecular density and turnover markers. Integrating biomechanical analyses and high-resolution imaging could clarify how antiresorptive therapies modify stress distribution and microarchitecture of periprosthetic bone [47]. Furthermore, sequential or combined therapy regimens should be explored: the use of bisphosphonates after discontinuation of denosumab is recommended to prevent rebound, but there are no studies evaluating whether this strategy influences implant stability [15]. Other areas of interest include the identification of biomarkers of risk for prosthetic mobilisation and evaluation of the impact of new prosthetic materials and designs on bone response in the presence of antiresorptive therapy [48].
In conclusion, perioperative denosumab exposure was not associated with differences in the cumulative incidence of revision after THA but was associated with a higher revision incidence after TKA. This may reflect the drug’s potent antiresorptive effect combined with the mechanical demands of the tibial component. These findings suggest that alendronate may be associated with more favorable outcomes in TKA, while in THA, the choice of therapy can be tailored based on individual clinical factors. Further studies are needed to confirm these results and better understand the underlying mechanisms.



Comments (0)