
Remember me




A 72-year-old Caucasian male was admitted to the general surgery ward as an emergency to a district general hospital, presenting with four weeks of painless obstructive jaundice. The patient has previously been healthy with no diagnosed health conditions, no routine medications, no relevant family history and had not previously undergone any previous operations.
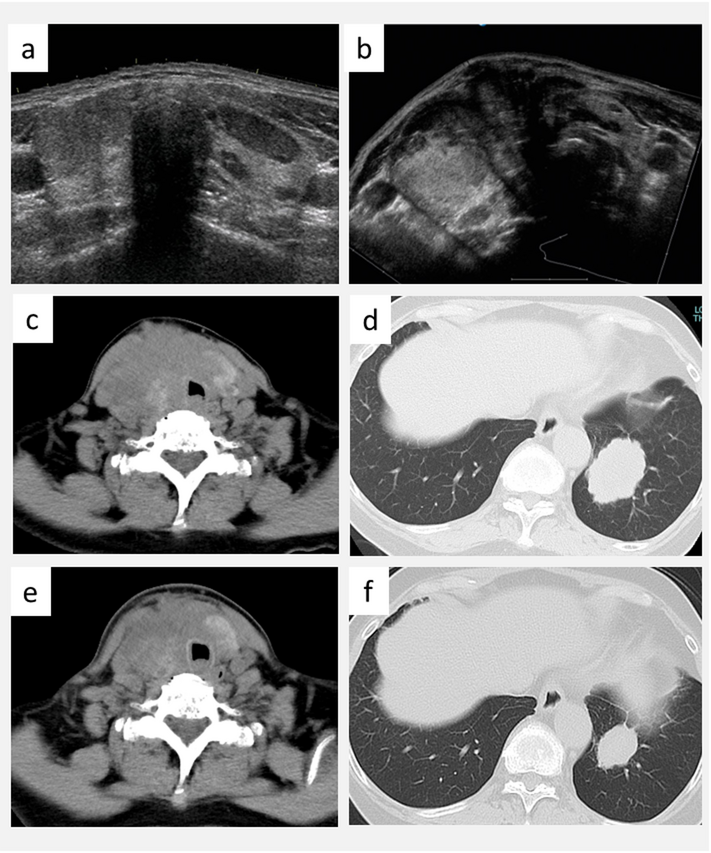
A thoraco-abdominopelvic computed tomography (CT) scan revealed a 15 mm filling defect within the distal common bile duct, accompanied by dilatation of both intrahepatic and extrahepatic biliary ducts (Fig. 1). There was no pancreatic duct dilation or evidence of a pancreatic mass. No other significant abnormalities were found on the CT scan.
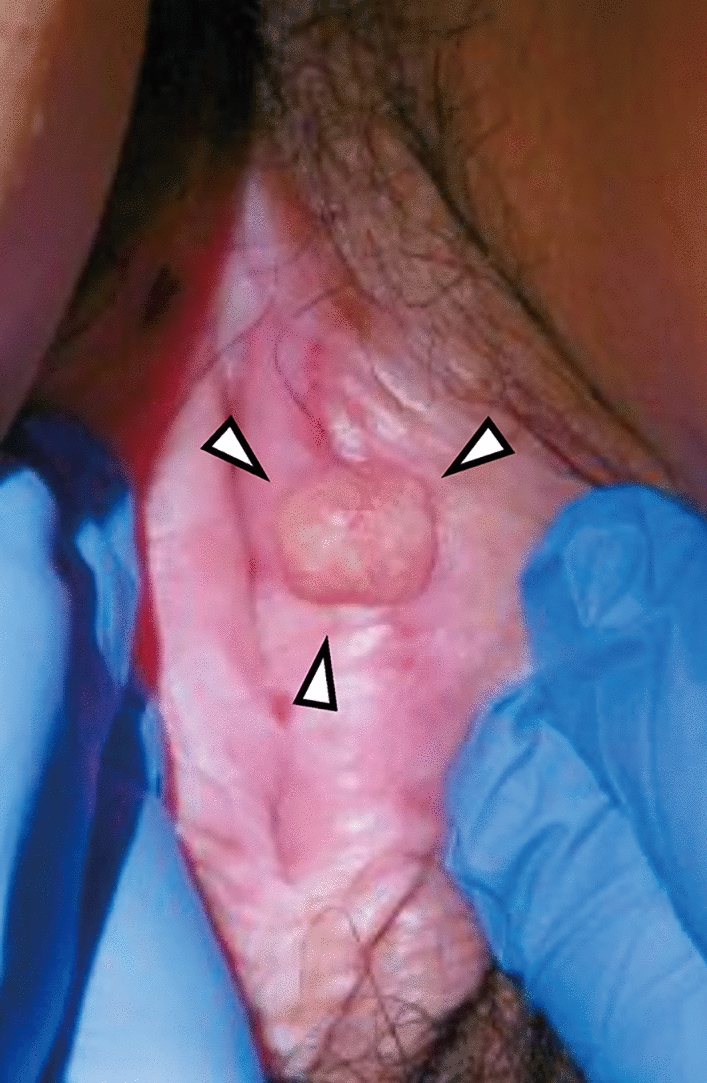
Magnetic resonance cholangiopancreatography (MRCP) confirmed biliary duct dilatation, revealing a solid mass measuring 19 mm longitudinally and 13 mm transversely, raising suspicion for malignancy (Fig. 2). An endoscopic retrograde cholangiopancreatography (ERCP) was attempted twice but was unsuccessful due to the inability to cannulate the common bile duct due to tumour involvement. Following this, the patient was transferred to our unit at Glasgow Royal Infirmary, after 10 days from initial admission at the district general hospital.
Fig. 1 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.Coronal portal venous phase CT showing abrupt truncation of the distal CBD with 2.4cm stricture/intraluminal soft tissue which extends to the level of the ampulla, as indicated by the arrow. Associated moderate upstream intra and extrahepatic biliary tree dilatation is present
Fig. 2 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.Coronal T2 SPACE MRI confirming distal CBD stricture as indicated by the arrow, with upstream biliary tree dilatation. Normal calibre main pancreatic duct suggests the mass originates within CBD rather than from the pancreas or ampulla
Laboratory tests on admission revealed significant abnormalities: alkaline phosphatase was elevated at 215 U/L, total bilirubin was markedly increased at 439 µmol/L, AST was 140 U/L, ALT was 164 U/L, and albumin was low at 27 g/L. Serum levels of carcinoembryonic antigen (CEA) and carbohydrate antigen (CA) 19-9 were within the reference range. The amylase level was mildly elevated at 157 U/L, and C-reactive protein (CRP) was raised at 39 mg/L. These results are presented in Table 1.
Table 1 Laboratory and tumour marker results obtained upon the patient’s admission to our unit, prior to stentingConsequently, an endoscopic ultrasound-guided stenting of the bile duct was performed using a lumen opposing selfexpanding Metal Stent (SEMS), resulting in the complete resolution of bilirubin levels and a marked improvement in albumin levels to 33 g/L. We conclude that the improvement in serum albumin levels following stenting is attributable to the resolution of the temporary acute phase response caused by obstruction by the polypoid mass, which had previously contributed to the mildly low albumin levels. The patient clinically improved following stenting and was discharged from our unit 6 days after admission. He did not develop renal impairment, coagulopathy, or change in neurological status throughout his admission.
Magnetic Resonance Imaging (MRI) of the liver showed no evidence of metastasis. Given the high suspicion of malignancy and without tissue diagnosis, the patient underwent a classic Whipple resection (pancreaticoduodenectomy), 6 weeks post-discharge of his acute admission. During the operation, no metastasis was identified, but extensive inflammation of the portal structures and intrahepatic biliary tree stones were noted. The surgery had proceeded without the use of neoadjuvant chemotherapy or radiotherapy following multi-disciplinary team (MDT) decision, as the tumour was perceived resectable, and the patient was deemed fit and healthy with no comorbidities.
Pathological evaluation of the specimen demonstrated a Whipple pancreaticoduodenectomy specimen comprising stomach (40 mm along the greater curvature and 30 mm along the lesser curvature), small bowel (190 mm), pancreatic head (100 × 55 × 20 mm), attached common bile duct (40 mm), and cystic duct (25 mm). A separate gallbladder measuring 75 × 30 × 30 mm and omentum measuring 330 × 95 × 15 mm were also submitted.
On sectioning, a pale tumor was identified centered in the distal common bile duct, measuring 34 × 10 × 25 mm, with focal extension into the pancreas. A metallic lumen stent was present within the proximal common bile duct. The tumor exhibited a nodular configuration with solid architecture, demonstrating exophytic growth into the bile duct lumen and extension into the bile duct wall to a depth of 7.4 mm. Gross photographs of the resected specimen were unavailable due to institutional archiving limitations.
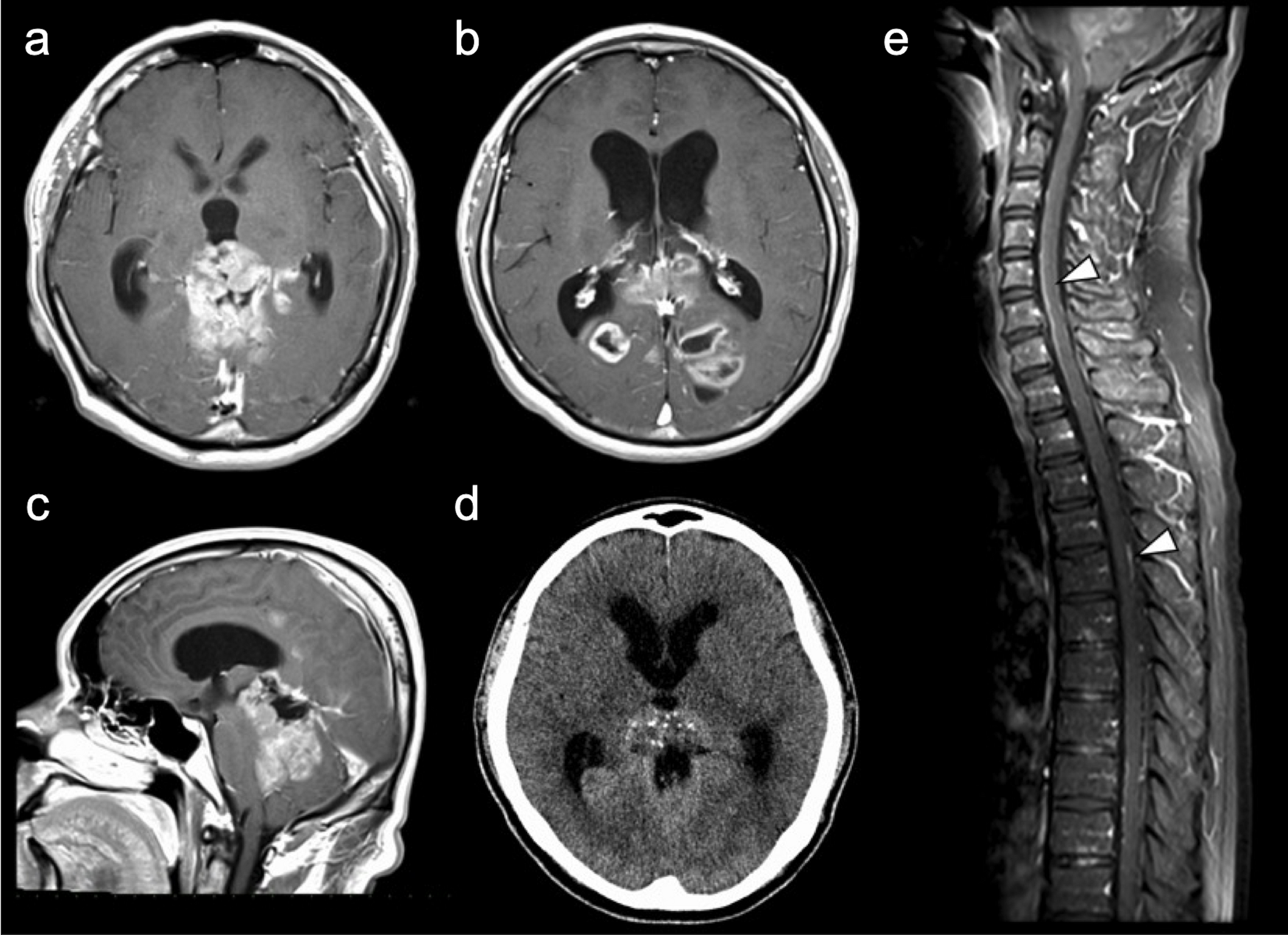
Histological examination revealed large, pleomorphic, spindle-shaped cells, along with angulated glands lined by biliary epithelium, exhibiting nuclear enlargement and prominent nucleoli (Fig. 3). Distinguishing between areas of glandular differentiation and entrapped background epithelium proved challenging. Specimen confirmed an R0 resection. A total of 18 regional lymph nodes were retrieved and histologically examined, including a separately submitted station 8 A lymph node. No metastatic carcinoma was identified in any of the examined nodes (0/18), corresponding to pN0 disease.
Fig. 3 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.This micrograph demonstrates a tumour predominantly composed of spindle cells with pleomorphic hyperchromatic nuclei. The architecture indicates sarcomatoid differentiation, with regions showing ambiguous glandular structures that are challenging to distinguish from entrapped background epithelium
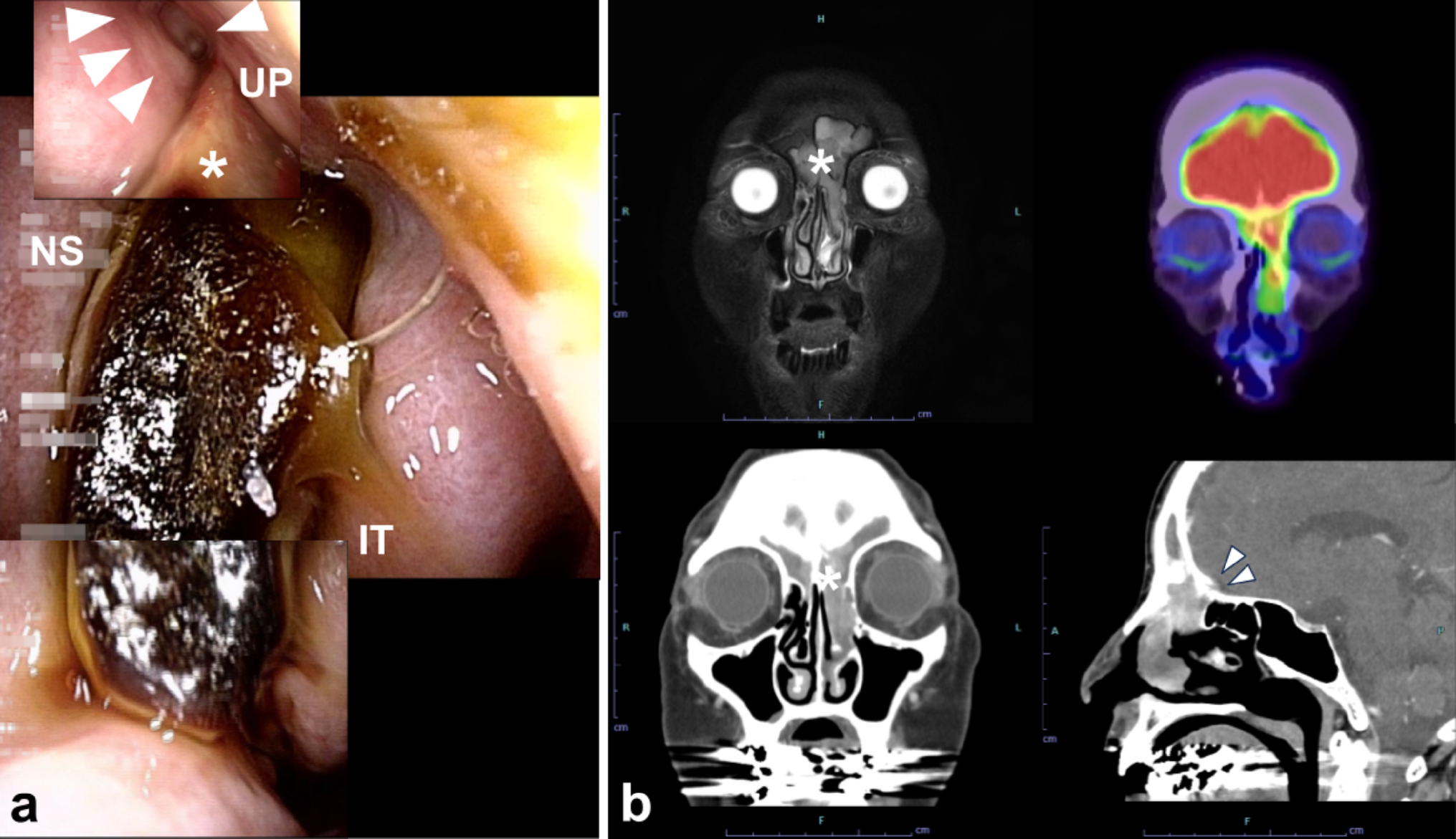
Immunohistochemical staining showed patchy expression of AE1/3 (Fig. 4) and CAM5.2 (Fig. 5), with focal cytokeratin MNF16 positivity, while all other markers; including CD34, CD56, Desmin, DOG1, MyoD1, S100, smooth muscle actin (SMA), STAT6, synaptophysin, anaplastic lymphoma kinase (ALK), CD1a, CD68, and langerin were negative.
Fig. 4 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.Immunohistochemical staining for AE1/3 demonstrates expression of the gene by spindle cells, confirming epithelial origin. The arrow points at a group of spindle cells that show strong expression of AE1/3
Fig. 5 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.Immunohistochemical staining for CAM 5.2 demonstrates expression of the gene by spindle cells, confirming epithelial origin
The extended immunohistochemical panel was employed to exclude important differential diagnoses. Negative ALK staining ruled out inflammatory myofibroblastic tumor [8], while STAT6 negativity excluded solitary fibrous tumor [9]. The absence of CD1a and langerin expression argued against histiocytic or dendritic cell neoplasms [10, 11], and negative lymphoid markers excluded lymphoma. Retained epithelial marker expression, including AE1/3 and CAM5.2, in combination with the histomorphological features, supported the diagnosis of sarcomatoid carcinoma. The lack of sarcomatous markers on staining directed us towards excluding carcinosarcoma as a diagnosis. The immunohistochemistry staining results are shown in Table 2.
Table 2 Immunohistochemical (IHC) staining profile of the resected specimen, summarising the expression of various markers, including cytokeratins, mesenchymal markers, neural markers, and other lineage-specific markers, detailed along with the corresponding antibody clone, manufacturer, heat-induced epitope retrieval (HIER) method, and dilution usedThe patient was diagnosed with Grade 3 sarcomatoid carcinoma, reflecting poor histologic differentiation, and stage T2 according to the TNM staging system of the American Joint Committee on Cancer (AJCC)/Union for International Cancer Control (UICC), 8th edition, for extrahepatic cholangiocarcinoma [12]. Chronic cholecystitis was observed in the gallbladder, along with a focal pancreatic intraepithelial neoplasia in the background pancreas.
The patient experienced no significant postoperative complications and was discharged 18 days post-surgery. As of the 16-month follow-up, there has been no recurrence of the disease, with the patient having returned to normal activities.
Comments (0)