A case of Ewing sarcoma in the frontal sinus of an elderly patient is presented. This case highlights two key considerations: first, sinonasal Ewing sarcoma may be misdiagnosed as other small round cell tumors, such as ONB; second, surgery or carbon-ion radiotherapy alone is unlikely to achieve curative outcomes without chemotherapy.
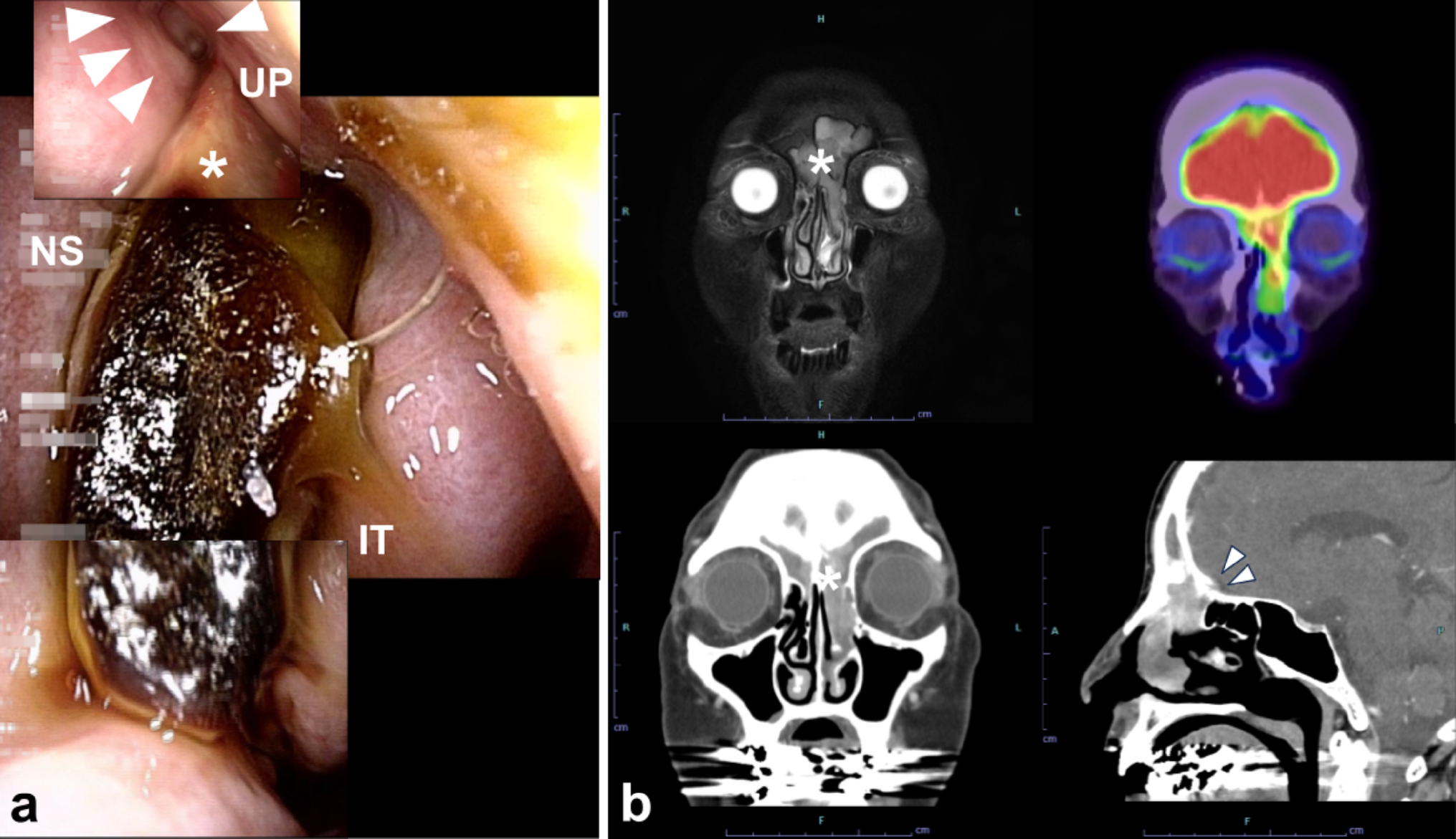
Making a pathological diagnosis of sinonasal tumor is not easy. Sinonasal tumors are often hemorrhagic and present with surrounding inflammatory mucosa. The limited amount of tumor tissue obtainable in an outpatient setting may not allow for the comprehensive staining needed to differentiate various tumors. In this case, the initial pathological diagnosis was ONB; however, endoscopy and imaging showed no tumor in the olfactory cleft, raising clinical suspicion of an alternative histological type. A larger tissue sample was eventually obtained under general anesthesia, enabling detailed histological evaluation with extensive IHC, and a definitive diagnosis of Ewing sarcoma was established by FISH. Ewing sarcoma is most common in adolescence or early adulthood, with only 6%–8.5% [4, 5] of cases in patients > 40 y and 1% in those > 60 y [4]. However, among 93 reported cases of sinonasal Ewing sarcoma [6,7,8,9,10,11,12], 7 (7%) were patients over 60 years old, suggesting a higher proportion of elderly patients in sinonasal cases compared with other sites(Table 1). Sinonasal Ewing sarcoma presents as a rapidly progressing tumor with nonspecific symptoms, such as nasal obstruction, epistaxis, and visual impairment. It has no characteristic imaging findings [6]. Ewing sarcoma is classified as a small blue round-cell tumor that may arise in the sinonasal cavities, along with other tumors such as ONB, neuroendocrine carcinoma, sinonasal undifferentiated carcinoma, rhabdomyosarcoma, malignant melanoma, and lymphoma [13]. The current definition of Ewing sarcoma encompasses sarcomas of small round cells that possess fusion between a member of the FET (typically EWSR1) and ETS gene families [2]. ONB is a sinonasal malignancy arising from the olfactory epithelium in the olfactory cleft. The predominant age range for ONB is between 40 and 60 y [14]. Misdiagnosis of ONB as other small round-cell tumors has been reported [15]. Currently, IHC and FISH assays facilitate the differential diagnosis. FLI-1 is positive in about 70% of Ewing sarcomas, whereas it is negative in nearly all ONBs [16]. Detection of a fusion gene is definitive for diagnosing Ewing sarcoma [2]. When Ewing sarcoma is not suspected, fusion gene testing may not be performed, leading to a misdiagnosis as ONB or other histological types. In cases where the pathological diagnosis conflicts with clinical findings, alternative histological types should be considered, and further pathological examination should be performed.
Table 1 Reported cases of sinonasal ewing sarcoma in patients aged over 60 yearsEwing sarcoma is highly metastatic. The standard treatment is a multimodality approach that combines systemic chemotherapy with local therapies such as surgery and radiotherapy. The chemotherapy regimen consists of vincristine, doxorubicin, and cyclophosphamide, alternating with cycles of ifosfamide and etoposide (VDC-IE). This regimen is highly toxic, making it difficult for many elderly patients to maintain dose intensity, leading to poorer outcomes [17]. Older patients are more likely to require dose reductions, particularly for doxorubicin, due to myelosuppression [18]. A subgroup analysis of a randomized controlled trial found the benefit of adding IE only in patients aged ≤ 17 y [19].
A case of Ewing sarcoma in the frontal sinus of an elderly patient was presented. The tumor initially was suspected to be ONB. While clinical information—such as the patient’s age, endoscopic appearance, and radiological findings—is generally important for pathological diagnosis, it is particularly essential for evaluating sinonasal small round-cell tumors. For sinonasal Ewing sarcoma, surgery followed by radiotherapy or definitive carbon-ion radiotherapy are insufficient. In elderly patients, intensive chemotherapy can be challenging. Developing optimal treatment strategies for elderly patients is therefore highly desirable.





Comments (0)