
Remember me




Cancer of Unknown Primary (CUP) is a metastatic malignant tumour whose primary site cannot be identified even after an intensive examination. It accounts for approximately 2%–5% of all malignant tumours [1]. Given that the primary site is unknown, administering systemic chemotherapy based on the type of primary malignancy is challenging, and the median survival time is extremely poor, typically approximately 6–12 months [1, 2]. Conversely, in patients with a favourable prognosis, where the primary site is strongly suspected based on the histological type, clinical features, and immunohistochemical (IHC) staining results, long-term survival may be expected with specialized treatment [3].
In CUP management, basic blood tests and relevant tumour markers are examined, and computed tomography (CT) and positron emission tomography (PET)-CT are performed to identify unrecognized malignant lesions. Subsequently, the histological type of the metastatic lesions is confirmed, and IHC staining is used to aid in identifying the primary site [4]. Particularly, for adenocarcinomas, a combination of markers such as GATA binding protein 3 (GATA3), thyroid transcription factor-1 (TTF-1), and caudal type homeobox 2 (CDX2), in addition to the cytokeratin (CK) 7, and CK20 expression patterns, plays an important role in enhancing the diagnostic accuracy [4]. These results may facilitate the induction of organ-specific treatments, when possible, rather than empirical chemotherapy [5].
Breast cancer basically affects women, but it occasionally occurs in men. Male breast cancer (MBC) accounts for < 1% of all breast cancers, and occult male breast cancer (OMBC) cases are extremely rare [6]. When the results of the IHC analysis suggest a mammary origin, diagnostic clues include negativity for CK20 and positivity for CK7, GATA3, gross cystic disease fluid protein 15 (GCDFP15), and mammaglobin [6, 7]. Furthermore, human epidermal growth factor receptor 2 (HER2) overexpression or gene amplification may indicate the indications for molecular targeted therapy [8, 9].
Our case primarily presents a poorly differentiated adenocarcinoma with unknown primary and multiple liver and bone metastases. After detailed examination including IHC, an occult breast cancer was strongly suspected. To the best of our knowledge, only a total of 14 OMBC cases have reported for 17 years since 2008. We report another rare case, along with a review of the relevant literature, to aid in the diagnosis and treatment of this rare entity.
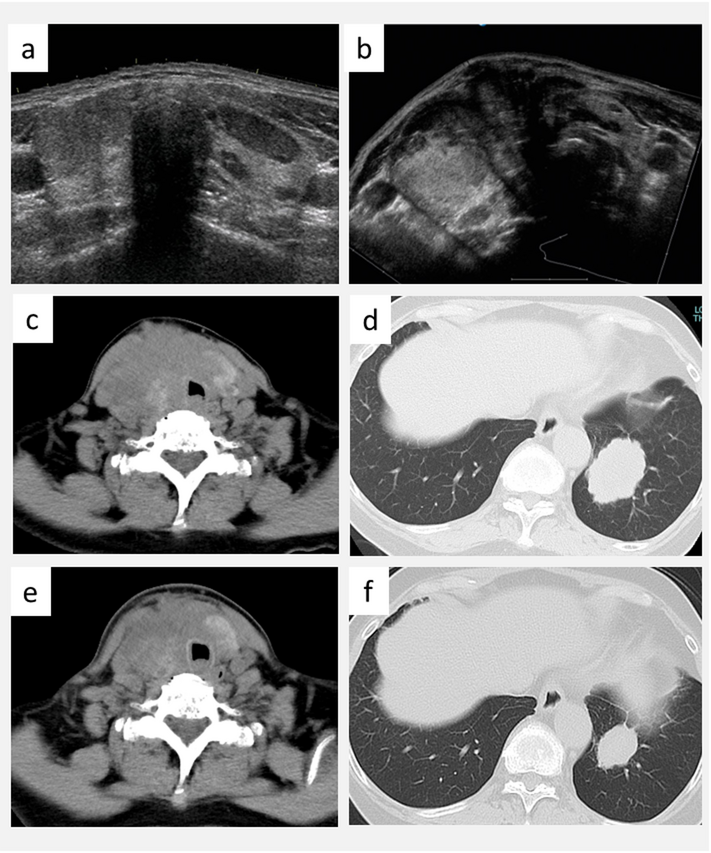
Case reportA 56-year-old man visiting Hospital X in July 2024 complained of lower back and bilateral leg pains. At the initial visit, blood tests revealed mild elevations in liver enzymes, and contrast-enhanced CT scans showed multiple mass lesions centred on the liver S6 region (Fig. 1A). Additionally, bone scintigraphy and PET-CT confirmed multiple bone metastases, involving nearly the whole spine (Fig. 1B). A percutaneous biopsy of the liver tumour revealed a pathological diagnosis of a poorly differentiated adenocarcinoma (Fig. 2A), with IHC positivity for CK7 (Fig. 2B) and negativity for CK20. Given that the primary tumour was not identified at this time, he was referred to our department in September of the same year for the evaluation of CUP [1, 4].
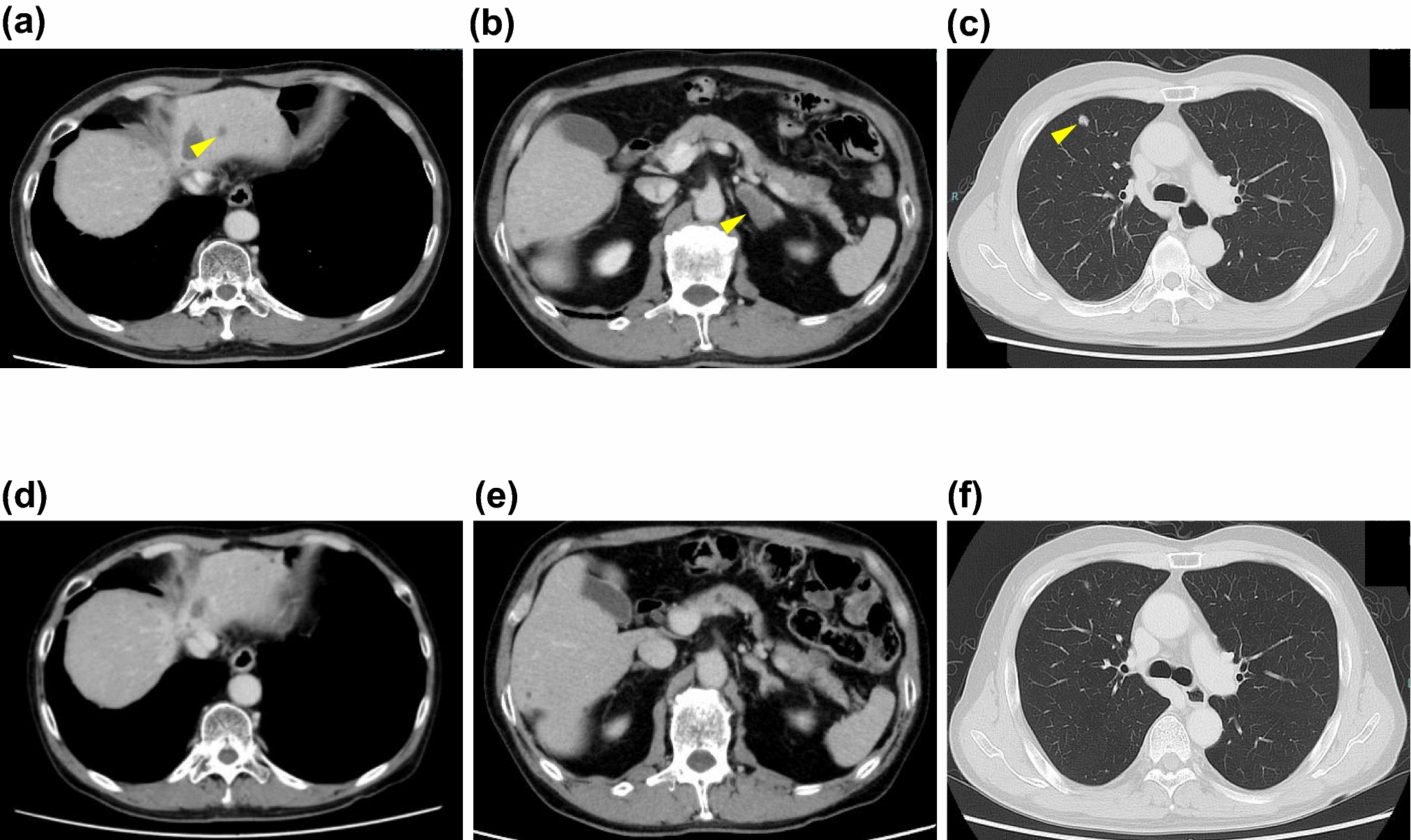
Fig. 1 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.Patient images. A. CT image at the initial examination. The black arrow indicates liver metastasis, and the red arrowhead indicates bone metastases. B. PET-CT image before chemotherapy. The regions with higher uptake of 18FDG signal are indicated in the liver and whole spine. C. CT image after five cycles of CBDCA + PTX treatment. Liver metastasis disappeared and the spotty osteolytic region was repaired. D. PET-CT image after eight cycles of CBDCA + PTX treatment. The uptake in the liver disappeared and the spine signals decreased. E. Mammography of the right breast. F. Mammography of the left breast. No tumour was detected in both breasts
Fig. 2 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.Histology and immunohistochemistry of the liver tumour. A. Haematoxylin and eosin (HE) staining. B. HE staining of the second biopsy after treatment. The black arrows indicate the residual tumour cells. C. PAS staining of the residual tumour cell. D. Immunohistochemistry (IHC) of the original liver tumour with anti-CK 7 antibody. E. IHC of the original liver tumour with anti-mammaglobin antibody (higher magnification). F. IHC of the residual tumour cells with anti-GCDFP15 antibody (higher magnification). G. IHC of the residual tumour cells with anti-androgen receptor antibody (higher magnification). The yellow arrows indicate the residual tumour cells. H. IHC of the residual tumour cells with anti-HER 2 antibody. The black arrows indicate the residual tumour cells. I. HER2 DISH of the residual tumour cells. The black bundle indicates HER2 gene amplification corresponding to 12 copies. The black dot indicates HER2 gene in the surrounding stromal cells. The pink dot indicates the centromere of chromosome 17. The black arrows indicate the residual tumour cells. J. IHC of the residual tumour cells with anti-PD-L1 antibody. The black arrows indicate the residual tumour cells
Although this diagnosis was later proven to be incorrect, the patient was initially diagnosed with CUP with multiple liver and bone metastases, and the prognosis at that time was considered to be poor. As the patient was living alone, his previous doctor advised him to return to his hometown where his relatives resided, and he was subsequently referred to our hospital.
At the initial visit in our hospital, the patient’s performance status was 1, he had mild weight loss (7 kg in 6 months), and his tumour markers were elevated (carcinoembryonic antigen: 94 ng/mL, cancer antigen 15–3: 305.6 ng/mL, carbohydrate antigen 19–9: 24.4 U/mL), but his PSA was within the normal range at 0.63 ng/mL, ruling out prostate cancer. CT and PET-CT scan revealed multiple tumours measuring < 6 cm in the liver, as well as multiple bone metastases to the spine through the cervical (C2) to the lumbar regions (L5) (Fig. 1A, B).
The current Japanese guidelines recommend that CUP treatment should be initiated within 1 month of diagnosis [5], but in the present case, nearly 2 months had passed since the initial consultation before treatment began. Owing to the difficulties in identifying the primary organ based on the pathological histology and rapid clinical progression, empirical chemotherapy with carboplatin (CBDCA, AUC = 3.5) and paclitaxel (PTX, 120 mg/m2) was selected [5, 8]. At 7 days after the initial administration, he developed grade 4 febrile neutropenia. The next day, he was diagnosed with sepsis and hospitalized. However, he recovered after treatment with granulocyte-colony stimulating factor (G-CSF) and carbapenem antibiotics. From the second treatment course onwards, PTX was continued at a 70% dose reduction. Treatment was performed approximately once a month, and polyethylene glycol-G-CSF was used in combination from the third treatment. To date, 13 treatment courses have been continued. Furthermore, the bone-modifying drug, denosumab, was administered every 4 weeks to treat bone metastases.
CT performed at the end of the third treatment course showed a significant reduction in liver metastases, with imaging findings suggesting a near-complete response (Fig. 2C). A PET-CT scan performed in April 2025 showed that the liver uptake had almost disappeared, the widespread spinal uptake had also been reduced to a spotty state, and bone metastasis appeared to be under control (Fig. 2D).
A subsequent detailed pathological examination revealed a poorly differentiated adenocarcinoma with cord-like, acinar-like, and tubular invasive proliferation of medium-to-large-sized adenocarcinoma cells with enlarged nuclei, condensed nuclear chromatin, and weakly eosinophilic cytoplasm, accompanied with fibrous stroma and inflammatory cell infiltration of lymphocytes, leading to a diagnosis of apocrine carcinoma (Fig. 2A). The pretreatment biopsy tissue was entirely consumed by IHC. An additional liver biopsy performed after chemotherapy revealed a considerable decrease in the tumour cell number (Fig. 2B). Periodic acid-Schiff stain (PAS) staining showed positive findings (Fig. 2C).
The IHC analyses revealed positivity for CK7 (Fig. 2D), mammaglobin (Fig. 2E), GATA3, GCDFP15 (Fig. 2F), and androgen receptor (AR) (Fig. 2G) and negativity for CK20. Furthermore, the examination revealed negativity for estrogen receptor (ER), progesterone receptor (PgR), thyroglobulin, TTF-1, paired box 8 (PAX8), p40, p63, CDX-2, CK5/6, and anti-hepatocyte specific antigen. The few remaining tumour cells in the additional liver biopsy showed strong HER2 3 + positivity (Fig. 2H), and HER2 gene amplification was confirmed by DISH (gene amplification: > 12, Fig. 2I) [9]. Based on the above-mentioned findings, our case presents an extremely rare occurrence of occult male HER2-positive breast cancer.
Programmed cell death 1 (PD-1) and programmed death-ligand 1 (PD-L1) were also positive (Fig. 2J). The patient’s combined positive score (CPS) was 30. All mismatch repair proteins were positive, indicating no mismatch repair deficiency. The IHC results are summarized in Table 1. These results suggested an occult male breast apocrine carcinoma (OMBAC). Additional mammography and breast ultrasound examination revealed no obvious abnormalities (Fig. 1E, F).
Table 1 Summary of the IHC staining resultsAntibodies (Abs) used in this case report were anti-CK7 Ab (SP52), anti-GATA3 Ab (L50-823), anti-mammaglobin Ab (31A5), anti-HER2 Ab (4B5), anti-GCDFP-15 Ab (EP1582Y), anti- CK20 Ab (SP33), anti-ER Ab (SP1), anti-PgR Ab (clone 1E2), anti-AR Ab (SP107), anti- PD-1 Ab (NAT105), anti-MLH1 Ab (M1), anti-MSH2 Ab (G21901129), anti-MSH6 Ab (SP93), anti-PMS2 Ab (A16-4), anti-TTF-1 Ab (TSSC3), anti-PAX8 Ab (MRQ-50), anti- p40 Ab (BC28) and anti-p63 Ab (4A4) were purchased from F. Hoffmann-La Roche, Ltd. (Basel, Switzerland). anti-PD-L1 Ab (clone 28–8) and anti-SMACA4/BRG1 Ab (EPNCIR111A) were purchased from abcam (Cambridge, UK). Anti-thyroglobulin Ab (8G7G3/1) and anti-Ki-67 Ab (MIB-1) from Agilent Technologies, Inc. (Santa Clara, California, U.S.), and anti-Ki-67 Ab (CDX2-88) from BioCare (Taoyuan City, Taiwan).
Following 1 year and 1 month after treatment initiation, no liver metastasis has been detected, bone metastasis remains under control, and treatment with CBDCA + PTX is still effective. If the patient’s condition deteriorates, anti-HER2 therapy (e.g. trastuzumab and pertuzumab) will be considered. Owing to the patient’s low cell count, cancer genome panel testing was not performed.
Comments (0)