Clinical utility of diagnostic laparoscopy for ovarian metastasis from breast cancer in a -mutated patient with hereditary breast and ovarian cancer syndrome: a case report and literature review
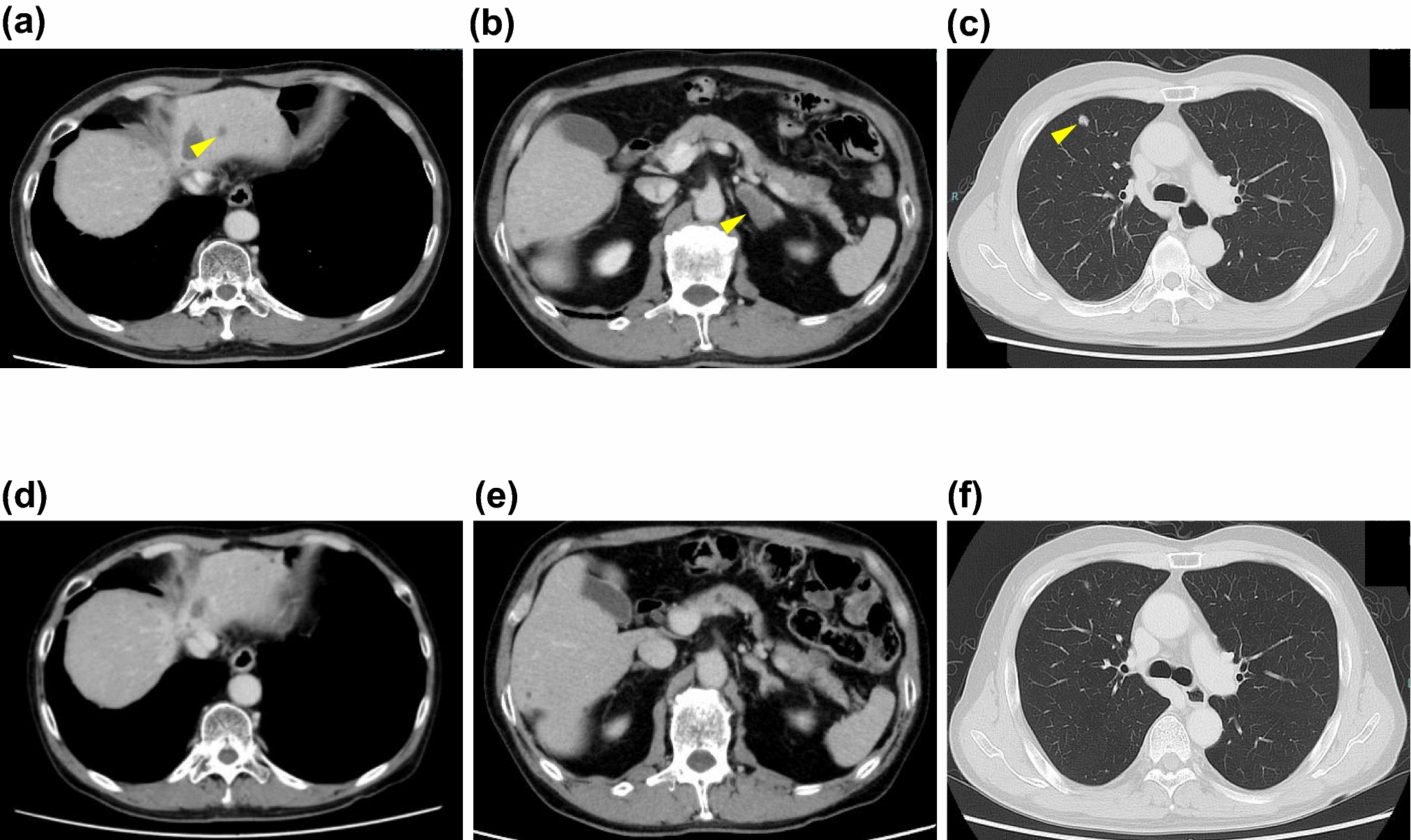
Ovarian metastasis from breast cancer has been reported in a substantial number of cases; however, reports that specifically document ovarian metastasis in the setting of hereditary breast and ovarian cancer syndrome remain limited. We describe a woman in her forties with hereditary breast and ovarian cancer syndrome caused by a germline BRCA1 mutation (c.117_118del) and a history of left-sided triple-negative breast cancer, invasive ductal carcinoma, clinical stage T1cN1M0, treated with mastectomy, adjuvant dose-dense epirubicin/cyclophosphamide and paclitaxel, followed by one year of maintenance therapy with olaparib. Two months after completion of olaparib, surveillance imaging identified bilateral ovarian masses with marked fluorodeoxyglucose uptake, peritoneal dissemination, and para-aortic lymph node enlargement, with elevated cancer antigen-125. Diagnostic laparoscopy with bilateral salpingo-oophorectomy revealed yellow serous ascites and multiple peritoneal nodules. Both ovarian tumors showed adenocarcinoma composed of small nests and cords. Sections prepared using the Sectioning and Extensively Examining the Fimbrial End protocol showed no serous tubal intraepithelial carcinoma. Immunohistochemical staining revealed CK7 and GATA3 expression, but no CK20, PAX8, WT-1, AR, ER, PgR, or HER2 expression. These results support a diagnosis of ovarian metastasis from the patient’s prior triple-negative breast cancer. Cytologic examination of ascitic fluid was negative for malignant cells. This case highlights that, in patients with hereditary breast and ovarian cancer syndrome and a history of breast cancer who present with ovarian tumors, both primary ovarian cancer and metastatic breast cancer should be considered. Diagnostic laparoscopy with pathologic and immunohistochemical evaluation provides a definitive diagnosis, helps avoid unnecessary cytoreductive ovarian cancer surgery, and supports timely initiation of breast cancer-directed systemic therapy.





Comments (0)