
Remember me
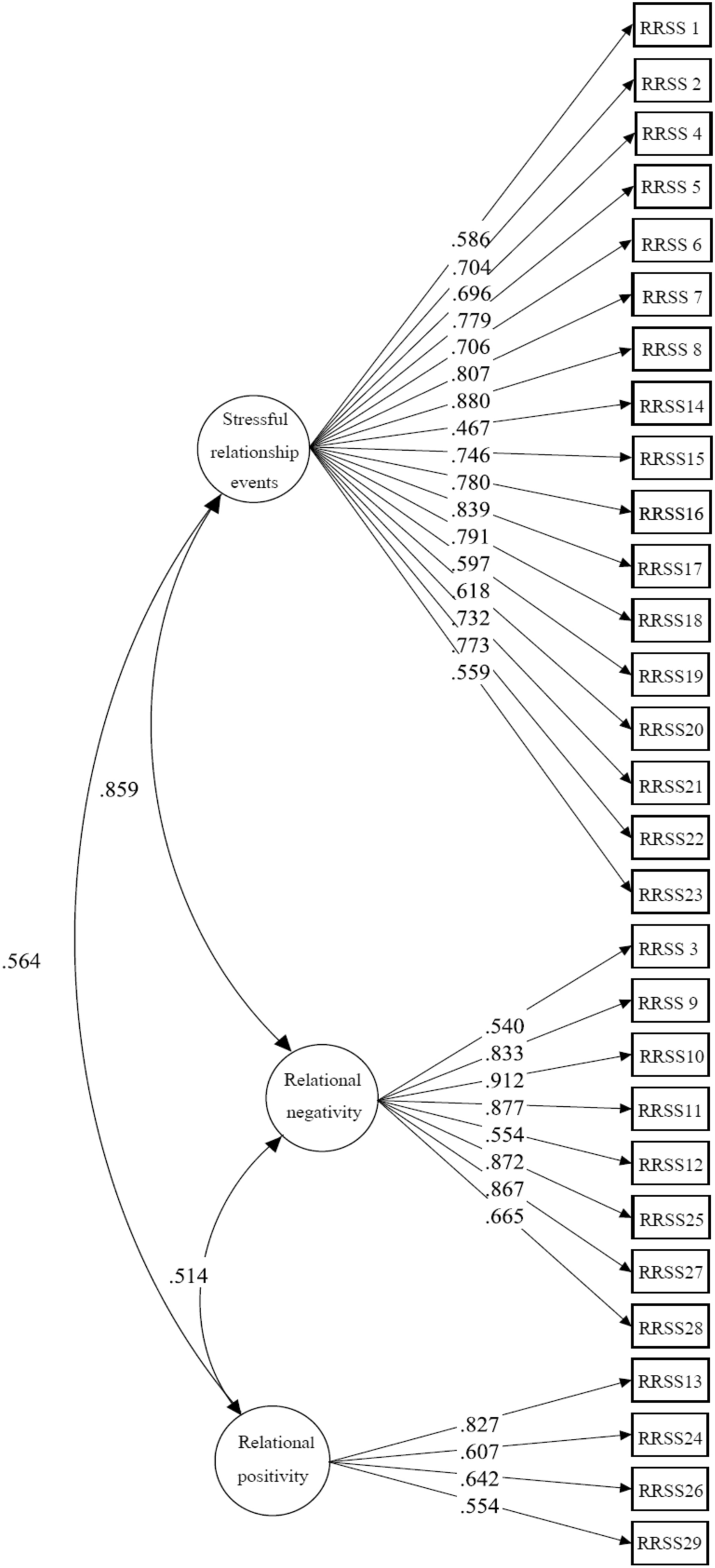
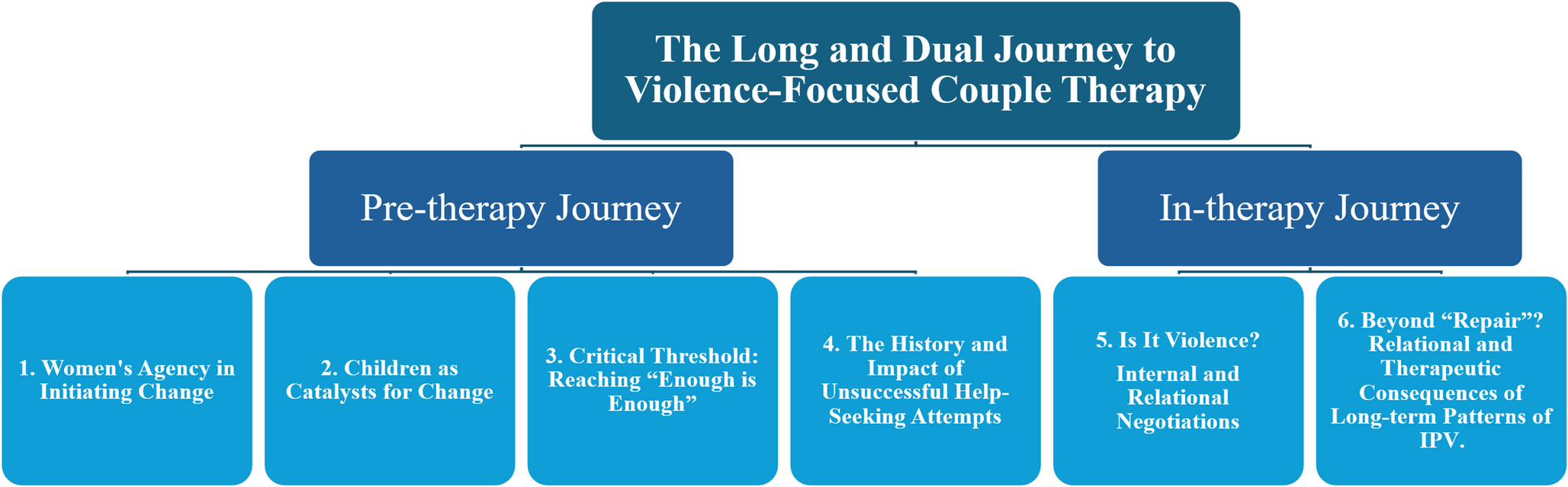
This study illuminates the complex, multilayered help-seeking processes of couples entering couple therapy, where IPV only becomes an issue after therapy has begun. Based on our results, we propose a Dual Journey Model, which captures both the Pre-therapy Journey (themes 1–4) and the In-therapy Journey (themes 5 & 6), two stages that are chronological yet iterative, reflecting how past experiences continuously shape in-session dynamics and vice versa, visualized in Fig. 2 below:
Fig. 2
Illustration of the Dual Journey Model
The pre-therapy journey refers to the often long and complex process that precedes therapy. It includes living with the effects of violence, acknowledging the problem, navigating formal and informal support systems, and reaching a state of readiness to seek help. This process is often marked by ambivalence, fear, previous unsuccessful attempts at help-seeking, and concerns about the children. In our study, these challenges typically unfolded over months or years, leaving behind a layered history of emotional distress and relational disruption that culminated in a critical threshold, often described as a point where “enough is enough.” These lived experiences are not left at the door when entering therapy; instead, clients bring them into the process, influencing their expectations, engagement, and interactions among participants during the in-therapy journey.
The in-therapy journey occurs within the therapeutic relationship and the couple therapy setting itself. In this study, it encompasses efforts to establish safety, build a working alliance, and identify and make sense of the violence as it is experienced and expressed. Importantly, it also involves fostering a shared and negotiated commitment to change, where violence is not seen as a peripheral concern but acknowledged as central to the therapeutic process. In this sense, if the in-therapy journey is to lead to violence-focused couple therapy in practice, it must involve collaborative negotiation and the co-creation of new relational meaning, supporting the emergence of a sufficiently shared understanding of the violence, its consequences, and a unified goal for the therapeutic project.
Drawing on Gadamer’s hermeneutic-phenomenological philosophy (Gadamer, 1998), the Dual Journey Model rests on the idea that our understanding is always shaped by our situated horizon of understanding that integrates past, present, and anticipated future. Within this setting, it means that clients and therapists make sense of what emerges not in isolation, but in connection with what has already been lived and what may yet become possible. For instance, when the therapeutic dialogue contributes to internal and relational negotiation of naming and framing violence, this does not simply state what has happened. Instead, it may reshape how past actions and situations are interpreted. What was once described as “he just hit the wall” or “anger” may be understood as a single act of material violence, or as part of a broader pattern of coercive or psychological abuse.
This retrospective re-interpretation, enabled by new language and understanding through dialogue and reflection, can reshape how clients understand their history, recalibrate their experience of the present, and expand and influence their sense of future possibilities, including critical decisions about staying in or leaving the relationship.
At the same time, pre-therapy experiences, such as mistrust, concern for the children, or doubt about the continuation of the relationship, can resurface in-session in either their original form or nuanced variations, shaping clients’ expectations, therapeutic dynamics, and possibilities during the in-therapy journey. The in-therapy journey may provide new language and a relational context through which earlier experiences can be re-evaluated. Thus, the pre- and in-therapy journeys are in this sense not merely sequential stages, but co-constitutive movements that continuously inform and reshape one another as therapy unfolds.
This Dual Journey Model is not merely descriptive; it serves both analytic and practical functions. For therapists, it offers a structured yet flexible tool for case conceptualization, enabling greater attunement to the evolving interplay between prior experience and current therapeutic dynamics. For service developers and policymakers, the model provides a scaffold for designing services that are responsive to the relational complexity and needs of couples who experience IPV, particularly those who do not disclose violence at intake for various reasons. In the following section, we outline some clinical implications for therapists, along with broader organizational and policy considerations.
Clinical Implications for TherapistsOur results point to several clinical implications for therapists working with couple therapy in the context of IPV. While therapists are well aware that clients bring a lived history into therapy, the Dual Journey Model calls for more active and deliberate attention to how this history shapes and is in turn shaped by the therapeutic process. Rather than treating the past merely as background information, therapists are encouraged to remain attuned to how each partner’s pre-therapy experiences continue to influence their engagement, sense of safety, capacity to speak about violence, and possibilities for change. Attending closely to how these experiences and relational patterns unfold within therapy may foster a more grounded and responsive approach to addressing IPV in couple therapy.
Revisit the Pre-therapy Journey Early onThis study’s results remind us that therapy does not begin as a blank slate. Couples carry various experiences from the pre-therapy journey, such as prior help-seeking attempts, which shape their expectations and engagement (Tambling et al., 2014). In low-threshold services like NFCS, where intake information is limited, therapists might more effectively engage with clients by revisiting their pre-therapy journey experiences and acknowledging and incorporating them into the in-therapy journey. By addressing themes such as failed interventions, ambivalence about staying together, and concerns for the children, therapists can help co-construct a shared understanding of why the couple is in therapy and what is at stake. This early attention to pre-therapy dynamics may lay the groundwork for safety and openness, while ensuring that the issues addressed in the in-therapy journey are meaningful and relevant to the couple.
Address Gendered Asymmetries in Engagement and ResponsibilityIn line with previous research, our data show that women most often initiated help-seeking, highlighting persistent gendered dynamics in who carries the responsibility for relational repair (Addis & Mahalik, 2003; Trillingsgaard et al., 2019). Such patterns illustrate how individual behaviors are embedded in broader gendered power structures (Dobash & Dobash, 2017; Kimmel, 2002), underscoring the need for therapeutic approaches that critically address asymmetrical structures. Feminist scholarship has long shown that women’s disproportionate assumption of emotional responsibility reflects broader cultural scripts of gendered care work, as for example conceptualized by Hochschild (2022) as emotion work, which can perpetuate inequities in both intimate relationships and therapeutic settings. Recognizing this dynamic is therefore essential to avoid unreflective reproducing structural asymmetries in the therapeutic process. If left unexamined, such asymmetries may reinforce unequal emotional labor and accountability within the therapeutic process, especially when one partner has used violence. Therapists may benefit from remaining attentive to how gendered relational scripts shape the dynamics of the in-therapy journey, particularly in terms of engagement and responsibility-taking, and implement interventions that redistribute the emotional and relational burden and responsibility (Knudson-Martin, 2013; Vall et al., 2018). At the same time, the gendered and relational patterns observed in this study must be understood within a broader Norwegian and Nordic cultural context characterized by ideals of equality, shared parenting, and mutual responsibility. While such egalitarian ideals can foster openness and collaboration in therapy, they may also obscure ongoing power imbalances and subtle forms of coercion that persist beneath discourses of equality (Wemrell et al., 2022). Therapists must therefore remain attentive to how these local cultural narratives around gender, conflict, and responsibility shape how clients describe, interpret, and respond to violence in their relationships.
Focus on the ChildrenChildren often act as both motivators for help-seeking and as therapeutic resources. In our study, awareness of and acknowledgment of the impact on their children frequently triggered “constructive distress,” encouraging parents to participate and seek help (Darwiche et al., 2022). Similarly, Merchant and Whiting (2018) found that many couples identified a “turning point” related to their children, such as witnessing a violent episode or reflecting on intergenerational transmission of violence, which served as a wake-up call to reconsider “where the relationship was headed.” In their grounded theory of desistance, moments when children observed violence or when parents saw its impact on them often triggered reflection, remorse, and a deliberate choice to change. At the same time, our study also indicated that uncertainty and fear of triggering child protection services led some individuals to withhold or soften their disclosures. This underscores the importance of a transparent and child-sensitive approach. Therapists should communicate clearly about their role, the limits of confidentiality, and the possible implications of disclosure, while also acknowledging the potential value of integrating a child-focused perspective in therapy or, in some cases, involving children directly when it can be done safely and meaningfully. Including children’s perspectives may deepen understanding of their situation (Holt et al., 2008) and strengthen motivation for change (Cravens et al., 2015; Merchant & Whiting, 2018). However, such involvement requires careful ethical consideration and clear information for all parties involved to ensure that participation fosters safety, trust, and therapeutic engagement.
Adjust the Pacing of Naming and Framing the ViolenceNaming and framing the main issue as violence was a negotiated process, both internally and relationally. Especially among men, there was a tendency both in the pre- and in-therapy journey to reserve labeling behaviors as violent, for overt physical acts. This finding aligns with earlier research on differences between clients and therapists in recognizing IPV (Dudley et al., 2008; Simpson et al., 2007). Therapists responded with dialogical flexibility, introducing language aligned with clients’ experiences and guiding them toward recognition and a shared vocabulary. This approach resonates with practice recommendations emphasizing careful pacing, screening, and sensitivity to escalation risk during conjoint sessions in IPV couple therapy (Keilholtz & Spencer, 2022; McCollum & Stith, 2008). Within the in-therapy journey, calibrated pacing is often essential when naming and framing the violence, striking a balance between the need for clarity and accountability, on the one hand, and fostering therapeutic engagement and a shared project for change, on the other. However, this process should not compromise the safety of those involved. At the same time, it is essential to recognize that naming violence may carry some risks. As Hearn (2013) has argued, naming violence can sometimes produce paradoxical effects, such as leading to minimization, justification, or a defensive reframing of responsibility, particularly when it threatens established gendered power positions or challenges dominant narratives of control. In this sense, therapists must remain critically attuned to how the timing, tone, and context of naming and framing violence can either open space for accountability and enhanced safety or, conversely, hinder it. Through ongoing, reflexive internal and external negotiations that remain sensitive to power, language, and lived experience, therapists can help transform the act of naming and framing violence as the core issue from a potentially polarizing intervention into a shared process that deepens understanding and supports safe, constructive change.
Long-term Violence and Emotional Exhaustion Can Limit the Potential for Relational Repair and Healing ProcessesIn such cases, reassessing the suitability of couple therapy becomes both ethically and clinically necessary (Snellingen et al., 2024). Within the broader literature, two dominant positions shape the discourse around how to approach IPV in couple therapy. The first position cautions against or rejects conjoint therapy when violence is present, citing concerns about safety, power imbalances, and the potential re-traumatization of victims. This position has been widely discussed and challenged in the literature (Armenti & Babcock, 2016; Hurless & Cottone, 2018; Stith & McCollum, 2011). The second position advocates for more differentiated clinical judgment, often guided by IPV typologies, particularly the distinction between coercive controlling violence and situational couple violence, as a basis for deciding whether conjoint therapy may be appropriate (Holtzworth-Munroe & Stuart, 1994; Johnson, 2008). Yet, others argue that such typologies, while clinically helpful, are often empirically inconsistent or overly rigid to fully capture the dynamic and evolving nature of couples’ lived experiences in therapy (Alexander & Johnson, 2023). Our results support this view; typologies may serve as heuristics but must be complemented by clinical judgment attuned to evolving relational dynamics. Therapists should continuously assess whether the couple is committed to a shared, regenerative process and whether conditions are safe enough for conjoint work (Snellingen et al., 2024). This involves ongoing monitoring of how the pre-therapy journey influences and integrates with the in-therapy journey, as well as critically evaluating how the in-therapy process is unfolding, shaping not only what is addressed in therapy but also how safety, trust, and change are made possible.
Organizational and Policy ImplicationsIn low-threshold, generalist services such as NFCS, where therapists begin with limited information, this study highlights several key implications for organizational and policy development. While the discussion draws on the Norwegian NFCS context, the implications are relevant to other service systems aiming to integrate violence-sensitive couple therapy, including those operating with different mandates, thresholds, or resource levels. These implications align closely with the results and emphasize the interdependence of clients’ pre-therapy experiences and the in-therapy process.
Facilitate Early Access To pre-therapy Journey ExperiencesServices should not rely solely on client self-disclosure of violence during early sessions. While some couples may feel ready and able to share their experiences early, many do not. To better support the in-therapy journey, organizations would benefit from proactively creating conditions for disclosure that are relevant for the specific service and that support and supplement the therapist’s clinical judgement. This may include some routine inquiries, structured intake protocols, and separate initial interviews, practices that enhance risk detection and support safer entry into therapy (Bograd & Mederos, 1999; Bradford, 2010; Schacht et al., 2009; Zahl-Olsen et al., 2019).
Systematically Develop and Continually Cultivate Therapists’ Capacity To Address IPVServices should support therapists in building capacity to address and manage IPV in couple therapy. Even with routine inquiry and screening in place, as our results indicate, many clients might not initially recognize their behavior as violent or be ready to disclose. Couple therapists need training that goes beyond generic knowledge and typology labels, providing them with skills to sensitively introduce, reframe, and revisit issues related to IPV in couple therapy, as it may emerge gradually, ambiguously, or in fragmented form. These capacities can be strengthened through ongoing supervision, specialized training, and an organizational culture that scaffolds reflective and ethically grounded practice (Sammut Scerri et al., 2017; Snellingen et al., 2024). For therapists and organizations that choose to continue working conjointly after violence has been disclosed, a range of models and frameworks have been developed to support safe and differentiated clinical practice (Cooper & Vetere, 2008; Keilholtz & Spencer, 2022; Sammut Scerri et al., 2017; Slootmaeckers & Migerode, 2018, 2020; Stith et al., 2012; Vall et al., 2018). These approaches emphasize careful assessment of the type of violence, power dynamics, and motivation for change, alongside continuous monitoring of risk and safety throughout the therapeutic process. However, such competence cannot be assumed after short-term implementations; it must be continually cultivated, systematically supported, and embedded within both clinical routines and ongoing professional development structures if this work is to remain safe, effective, and sustainable over time (Husso et al., 2021).
Develop Dynamic Service Models that Evolve with the JourneyClients who enter therapy with complex pre-therapy histories, such as long-term IPV, negotiations about naming and framing the violence, ambivalence regarding continuing the relationship, concerns about children, or fragmented help-seeking, often require integrated and adaptable formats within the in-therapy journey. Services like NFCS would enhance their capacity to meet the needs of the clients by supporting transitions between individual, couple, and family modalities based on ongoing assessment. Flexibility across the therapeutic timeline, especially at key transitions and changes, can enhance safety, therapeutic relevance, and continuity (Littlechild et al., 2024; Stith & Spencer, 2024; Visser et al., 2020).
Prioritize Continuity of CareRepeated unsuccessful help-seeking can erode trust and diminish hope in therapy and services. Several participants described prior experiences of being misunderstood or offered services that did not fit their needs. These findings echo research linking past negative experiences with professionals to delayed help-seeking and guardedness (Tambling et al., 2014; Vogel et al., 2005). Especially in low-threshold services, maintaining continuity of care through clear routines, trauma-informed approaches, and transparent communication is essential. Services should outline structures and routines to ensure that clients are informed about what happens when violence is disclosed, including implications for safety, confidentiality, and follow-up. If couple therapy becomes unsafe or insufficient, services should be prepared to adapt, whether through format shifts, clarification sessions, or timely referrals. This “meeting clients where they are” approach strengthens ethical and safe support and responses, whether within the service or with corresponding help systems (Messing et al., 2015).
Strengths, Limitations, and Future ResearchThe results above should be interpreted as situated and illustrative rather than representative. In line with the epistemological underpinnings of IPA, the aim is not generalization but rather to provide a rich, idiographic account that can deepen understanding of how particular individuals make sense of their lived experiences (Smith et al., 2021). By attending closely to the meaning-making of participants within their relational and therapeutic contexts, the study provides insights that may resonate beyond the immediate sample through a form of “theoretical transferability” (J. A. Smith & Nizza, 2022). In this sense, the findings should be viewed as opening up possibilities for understanding rather than as definitive claims about all couples experiencing IPV in therapy.
A prime strength of this study lies in its multiperspective approach, which allows us to explore rich, relational nuances by examining therapist and couple perspectives simultaneously. Conducting interviews during ongoing therapy adds immediacy, allowing us to explore participants’ experiences as they unfold or in the near present. This enables us to examine multiple perspectives of both the past, present, and anticipated future from the vantage point of ongoing couple therapy, as well as the relationship between them. Our insider position within the NFCS seemed to facilitate trust and openness, encouraging deeper exploration.
However, this study was conducted within a Norwegian public couple and family therapy service, which offers low-threshold, accessible, and free couple therapy. The specific service context, combined with a small clinical sample and the highly experienced therapists included in this study, may limit the transferability of the findings to other settings. Adaptation may be needed in services with different structures, referral pathways, or levels of therapist capacity to address IPV. Our dual role as researchers and our work within the same organization may have influenced responses, despite participants reporting this as a sense of safety.
In addition, the recruitment process introduced certain limitations. Therapists observed that partners who had experienced or been subjected to violence were generally more willing to participate, whereas those who had used violence were more likely to decline. This imbalance may have influenced the diversity of couples represented in the data, as inclusion required consent from both partners and their therapist. Future research could therefore explore recruitment strategies or study designs that better capture a broader spectrum of couples affected by IPV.
Furthermore, the findings should be read in light of the Scandinavian sociocultural context, characterized by strong welfare-state and gender equality ideals that shape public understandings of family life and violence (Wemrell et al., 2022). Future studies could explore how cultural norms around emotional expression and gender intersect with help-seeking and disclosure processes more specifically in other cultural settings, where understandings of violence and responsibility may differ.
Future research could also extend to diverse services and clinical contexts to explore how both clients and therapists experience and make sense of the Dual Journey Model. Including couples dealing with varying forms of violence or relational challenges, as well as therapists with different levels of experience, may help assess the model’s adaptability and relevance across settings. Additionally, incorporating children’s perspectives could provide valuable insights into the broader relational dynamics and contribute to more ethically attuned practices in couple therapy.
Comments (0)