Intravenous Sotalol in Pediatric Intensive Care Patients With and Without Congenital Heart Disease: Hemodynamic and Antiarrhythmic Effects
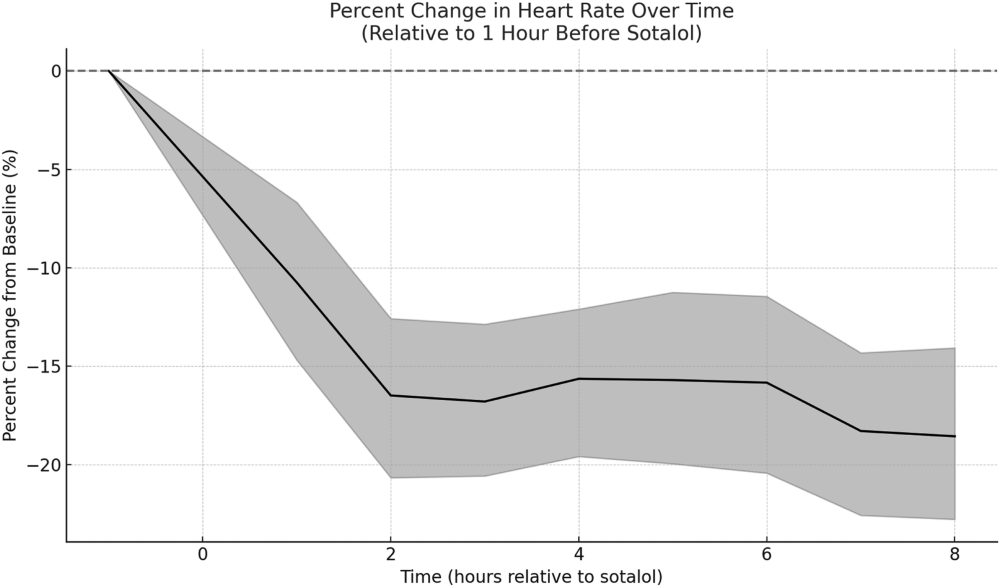
Sotalol is an antiarrhythmic with both class II and III properties, available intravenously since 2015. While its use in adults is well-documented, there is limited pediatric data. It has been used in pediatric patients for various supraventricular and ventricular tachycardias. This study aimed to characterize hemodynamic and antiarrhythmic changes following the first dose of intravenous sotalol in children with and without congenital heart disease. This single-center retrospective study included pediatric patients under 18 who received intravenous sotalol for the first time between January 2020 and January 2025. Data collected included age, congenital heart disease (CHD) status, univentricular circulation, electrophysiologic diagnosis, sotalol dose, dose discontinuation, corrected QT (QTc) interval change, and arrhythmia termination. Hemodynamic variables, including heart rate, mean arterial pressure, pulse oximetry, near infrared spectroscopy (cerebral and renal), central venous pressure, and vasoactive-inotropic score, were recorded at multiple hourly time points (1 h before to 8 h after dosing). Hemodynamic data were analyzed using the Friedman test, and longitudinal changes were assessed with a linear mixed effects model. The study included 112 patients with a mean age of 31.3 months. Of these, 60 (53.6%) had CHD and 15 (13.3%) had univentricular circulation. Of the 66 patients (59%) with active arrhythmias when receiving sotalol, 46 (70%) experienced arrhythmia termination or rate improvement with ability to pace. Heart rate significantly decreased from baseline at all time points (p < 0.01), with a 16% reduction within 2 h and an 18% reduction at 8 h. Arterial saturation increased by 1–1.4% at 6–8 h (p < 0.05). Mean arterial pressure, cerebral near infrared spectroscopy, renal near infrared spectroscopy, central venous pressure, and vasoactive inotrope score did not significantly change over time. These findings were not influenced significantly by other variables. The baseline QTc interval was 420.7 ± 65.4 ms and increased to 441.1 ± 46.7 ms post-dose (p < 0.01). Other hemodynamic variables showed no significant change. Intravenous sotalol was associated with stable short-term hemodynamic parameters in critically ill pediatric patients, supporting its safe use in the intensive care setting.




Comments (0)