
Remember me


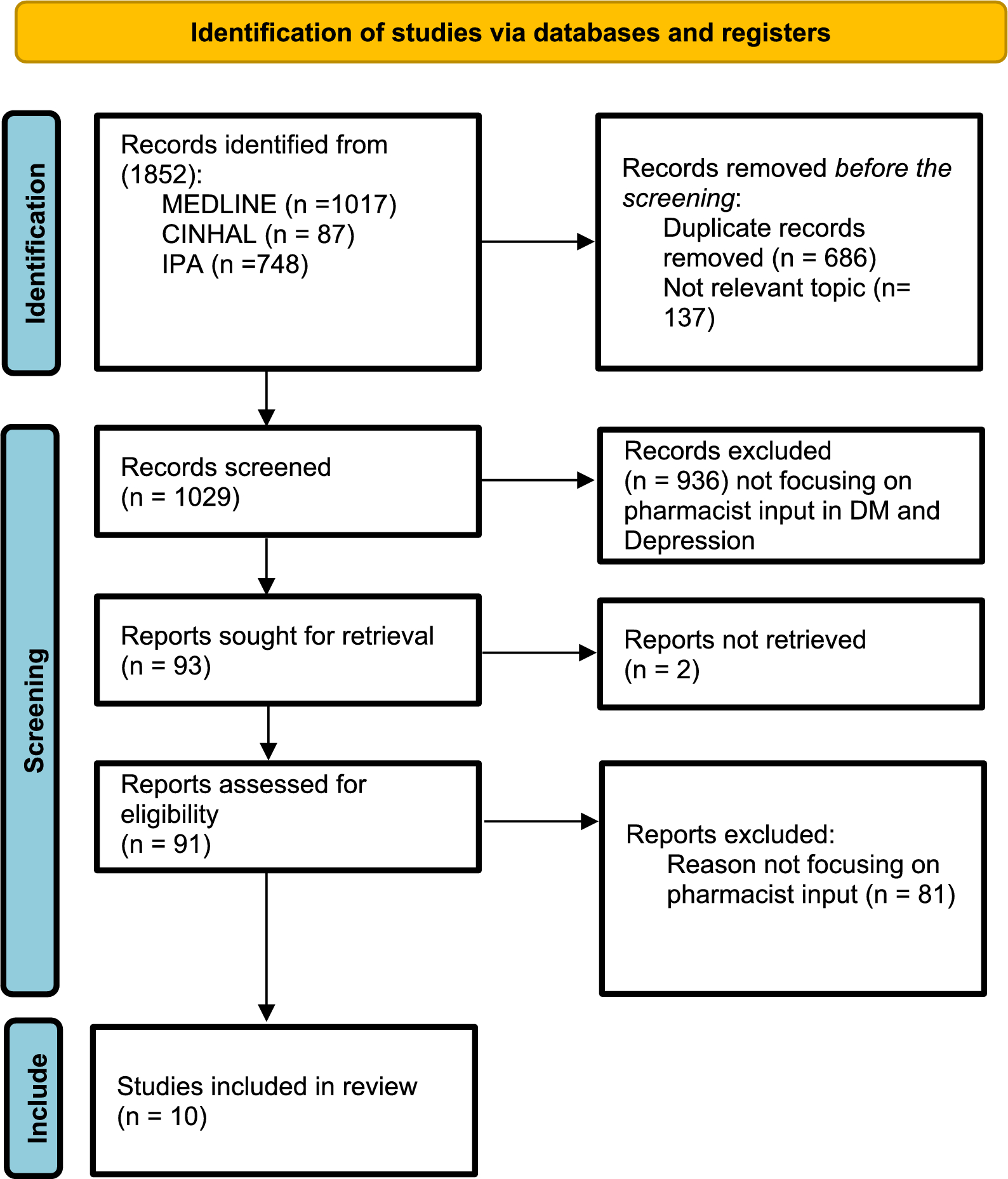
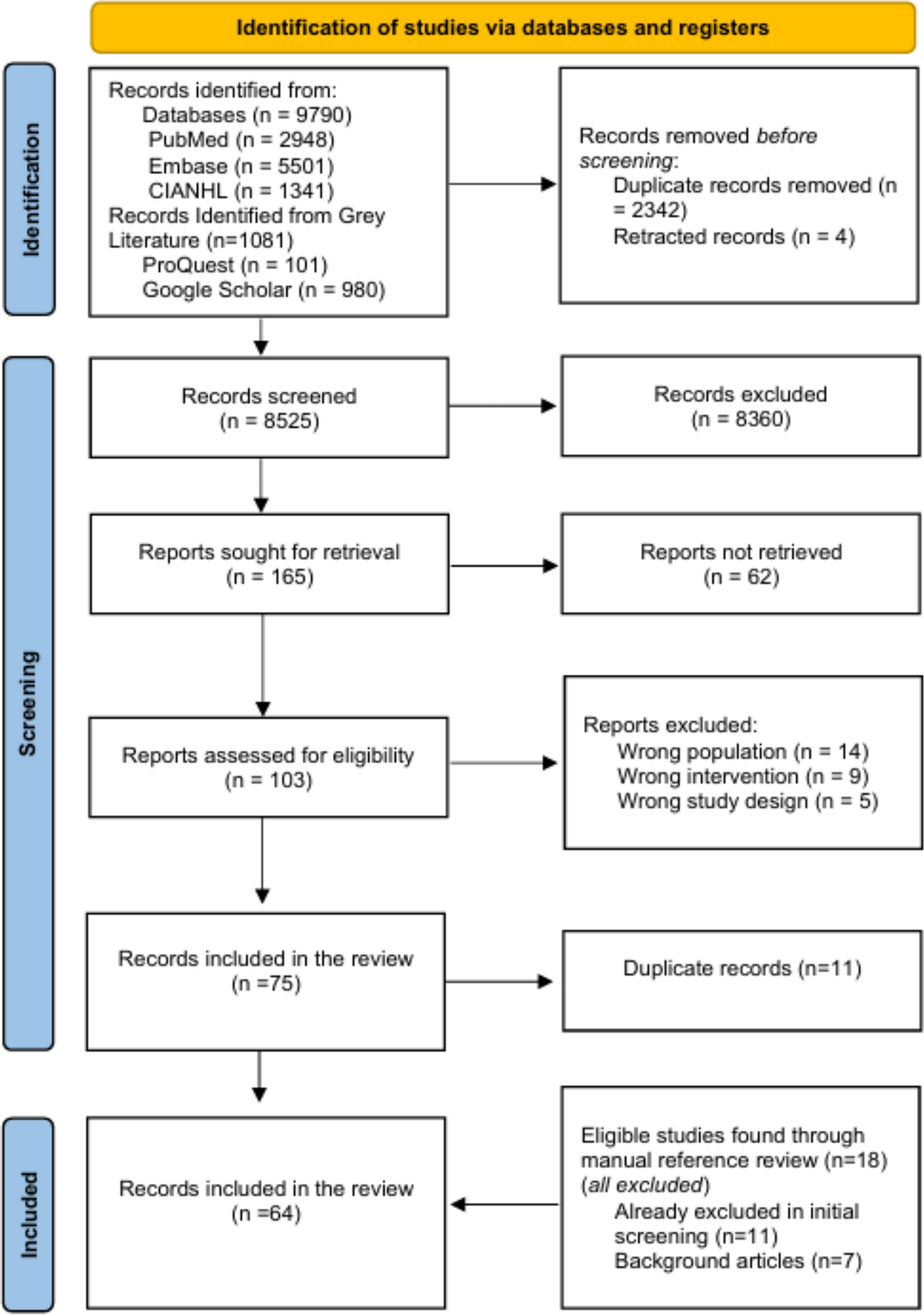
The systematic review identified 1852 records in MEDLINE, CINAHL, and IPA. Duplicate (n = 686) and nonrelevant records (n = 137) were manually removed, and 1029 records remained for screening. Additional screening of titles and abstracts further excluded 936 records, which did not focus on pharmacist input in depression connected to DM. Ninety-one records remained for full-text retrieval. Ten reports met the inclusion criteria and were included in the final systematic review (Fig. 1). No additional studies were identified through reference list or bibliography searches.
Fig. 1
PRISMA 2020 flow diagram for new systematic reviews that included searches of databases and registers only
Quality assessmentThe results of the quality assessment of all included studies (n = 10) with the MMAT tool are reported in Tables 1 and 2. The study designs were as follows: randomized controlled trials (RCTs) (n = 3) [23, 24, 31], ad hoc RCTs (n = 1) [25], retrospective cohort studies (n = 2) [28, 30], prospective cohort studies (n = 2) [27, 29], or cross-sectional studies (n = 2) [21, 26]. The quantitative descriptive studies (n = 6 of 10) were of optimal quality, particularly in terms of the research question, sampling strategies, measurement methodology, and response rate; however, a minor limitation was identified in one study with a small sample size, thus limiting the generalizability of the study [20]. (See Table 1). In the case of the RCTs, the quality assessment revealed limitations in the allocation concealment criteria in half of the studies. (Table 2) [21,22,23].
Table 1 Quality assessment tool for quantitative descriptive cross-sectional studies (MMATs)Table 2 Quality assessment tool for quantitative randomized controlled trials (MMATs)Data extractionAll reviewed reports (n = 10) were conducted in the United States (US). The participants included patients with diabetes mellitus (type 1 or type 2) or prediabetes with depression across various healthcare settings, such as community pharmacies [21, 24, 26], telehealth and outpatient clinics [20, 22, 25,26,27], Interventions were implemented either solely by pharmacists, by pharmacy students under the supervision of a staff pharmacist, or in collaboration with other healthcare providers. The sample size ranged from small (n = 15) [26] to large (n = 8,167) [27]; the duration of the studies ranged from a few months (n = 3 months) [25] to several years (n = 2.8 years) [24]. Of the 10 included studies, five focused exclusively on patients with type 2 diabetes [26,27,28,29, 32], three included both type 1 and type 2 diabetes [25, 30, 34], and two did not specify the diabetes type [31, 33]. Table 3 presents the results of the studies included in this systematic review, describing the role of pharmacists in medication therapy management, screening, and improving the quality of life in diabetic patients with depression, together with the main clinical outcomes.
Table 3 Overview of Clinical Characteristics and Main Clinical Outcomes, 2008–2025Pharmacist interventionsThe reviewed studies provided varied levels of detail regarding the pharmacist settings and recruitment. Two studies were conducted in community pharmacies [24, 28], while two utilized telehealth models to deliver pharmaceutical care [30, 31]. An additional six studies took place within outpatient clinics or primary healthcare centers [21, 23,24,25,26, 28]. Within these settings, in five studies, pharmacists were involved in screening for depression in individuals with diabetes or prediabetes [21, 25, 27,28,29], whereas in the other five studies, pharmacist interventions focused on managing already diagnosed depression among patients with diabetes. [23, 24, 26, 30, 31]. Pharmacy students under pharmacist supervision were involved in delivering interventions in two studies in primary care settings [21, 26], community pharmacists delivered another two [27, 29], a specialist psychiatric pharmacist led one intervention [28], and clinical pharmacists delivered five interventions in outpatient clinics [23,24,25, 30, 31].
The majority of patients were recruited through convenience sampling methods such as walk-ins [27] or proactive identification methods, such as patient chart reviews or direct invitations based on eligibility criteria [21, 23, 26,27,28,29,30,31]. In two studies, patients were referred through collaborative practice agreements [24, 25].
Process (care provided)Several pharmacists' interventions have been reported, with a primary focus on screening, medication management, and longitudinal follow-up. Depression screening was conducted in four studies via validated instruments: the Patient Health Questionnaire-2 and -9 (PHQ-2/PHQ-9 [27, 29], the Beck Depression Inventory-II (BDI-II) [26], and the Zung Self-Rating Depression Scale [21]. The studies focusing on depression management reported multicomponent interventions featuring medication optimization through comprehensive medication reviews and drug-related problem identification, pharmacist prescribing when dose adjustments were needed [25, 28, 30], and laboratory monitoring [31]. One study reported a lack of physician response, for some screened positive for depression using the PHQ-9, limiting the ability to assess the interventions’ impact [31]. Patient education components focused on therapeutic goal setting, diabetes self-management training, and weight control counselling [24].
Clinical outcomesScreening studies revealed a substantial prevalence of undiagnosed depression, with rates ranging from 19.8 to 42% among the studied populations. In most cases, participants are referred to primary care physicians for further evaluation and management [26, 27]. Follow-up audits indicated that a significant proportion of referred patients (60–70%) were initiated on treatment following these referrals [27, 29], whereas other studies reported the communication of screening results to primary providers without further intervention tracking [21, 28].
Six studies evaluated the outcome of pharmacist interventions in managing depression and diabetes in comorbid patients. Of them, two studies reported statistically significant improvements in glycemic control [24, 25], while, study reported measurable reductions in depressive symptoms in 89% of the patients and resolution in one-third of the patients [28]. One study revealed a greater HbA1c reduction in patients with depressive symptoms receiving pharmacist care (2.4 vs. 0.1 percentage points; P = 0.0081) but no change in depressive symptoms [25]. Comparative analysis indicated that pharmacist-led care was associated with increased adherence to glycemic and/or antidepressant medications in two studies [30, 31]. Two studies highlighted the role of pharmacists in identifying drug-related problems (DRPs), with tailored interventions resolving 84% of DRPs in one study [23] and an average of 11.7 identified DRPs per patient in another [25]. Notably, one study reported no clinically meaningful changes in glycemic control or depression severity following pharmacist intervention [31].
Comments (0)