Introduction
Severe cutaneous adverse reactions (SCARs) are rare but potentially life-threatening. Children and adolescents are especially vulnerable due to developmental pharmacology, immature immune systems, and limited premarketing safety data. However, large-scale evidence of drug-specific SCAR patterns in pediatric populations remains limited.
Aim
To investigate the epidemiology, clinical features, drug associations, and safety signals of SCARs in children and adolescents using the FDA Adverse Event Reporting System (FAERS).
Method
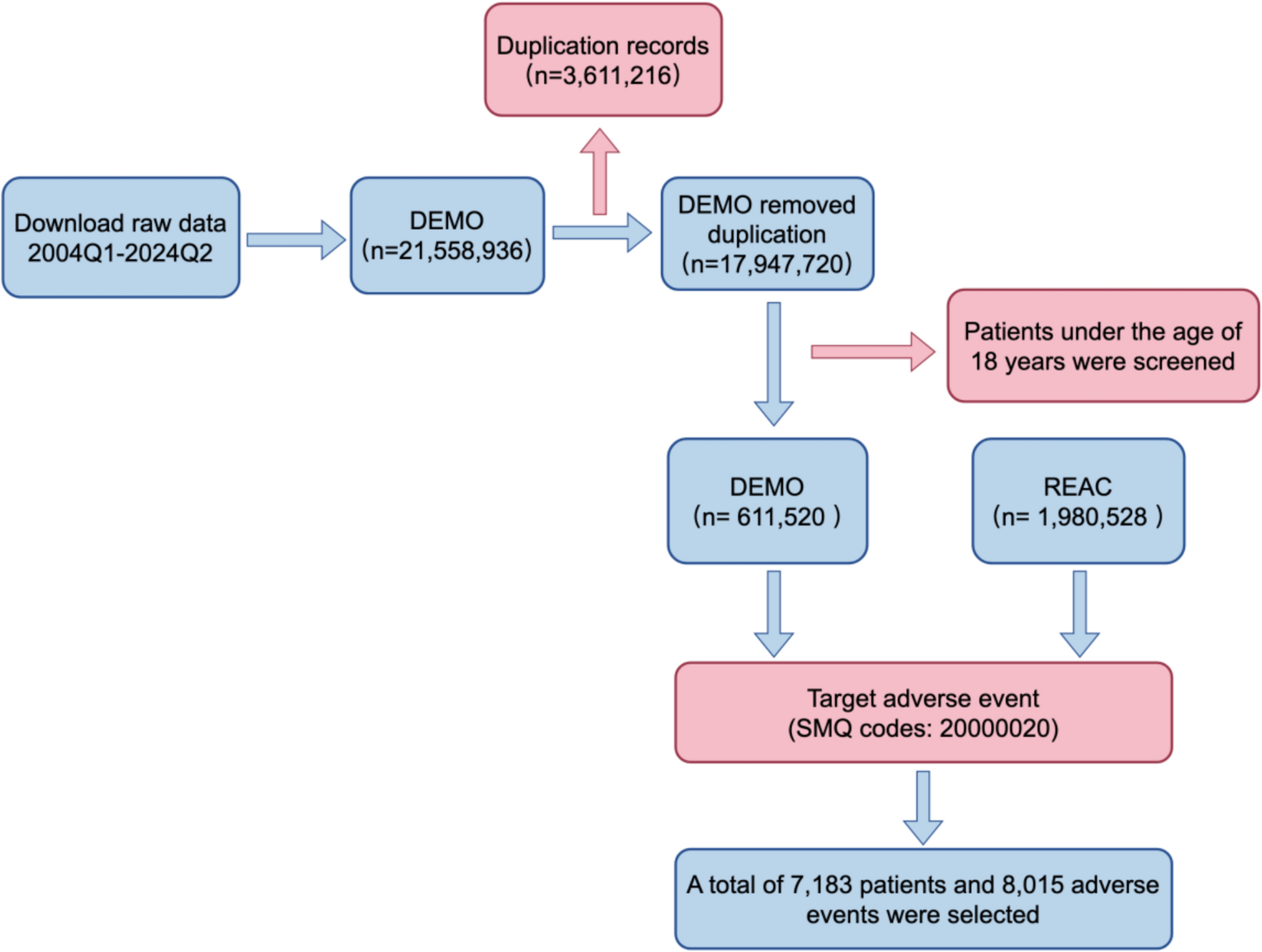
Reports of SCARs in patients aged ≤ 18 years were retrieved from FAERS from Q1 2004 to Q2 2024 and identified using narrow-scope Standardised MedDRA Queries (SMQs). Data cleaning followed the FDA-recommended procedures. Disproportionality analysis was performed using four methods: Reporting Odds Ratio (ROR), Proportional Reporting Ratio (PRR), Bayesian Confidence Propagation Neural Network (BCPNN; yielding Information Component, IC), Multi-item Gamma Poisson Shrinker (MGPS), and empirical Bayes geometric mean (EBGM). Drug-label reviews were used to compare the signal detection results with existing safety warnings.
Results
A total of 7183 pediatric SCAR reports were included. The number of reports has increased over time, with adolescents (13–17 years) and school-aged children (7–12 years) accounting for 68% of cases. The most frequently reported Preferred Terms were drug reaction with eosinophilia and systemic symptoms (DRESS; 32.5%), Stevens-Johnson syndrome (SJS; 27.9%), and toxic epidermal necrolysis (TEN; 19.0%). Hospitalization occurred in 64.5% of cases, and 6.3% were fatal. Among the 2005 cases with available onset time, 82.7% developed within 30 days of drug exposure. Thirty-eight drugs showed positive signals, including lamotrigine, phenytoin, sulfamethoxazole, and phenobarbital. Four drugs, ranitidine, anakinra, clonazepam, and rifampin, showed signals without corresponding warnings in the FDA pediatric labeling.
Conclusion
SCARs in children and adolescents show distinct patterns, high hospitalization and mortality, and strong links with antiepileptics and anti-infectives. Strengthening pediatric pharmacovigilance, implementing risk-alert systems, and promoting genotype-guided prescribing may help prevent these severe reactions.



Comments (0)