The Dortmund Maxillofacial Trauma Registry is one of the biggest monocentric databases worldwide, with over 14,500 individual patient datasets. The monocentric study has its advantages and disadvantages. A clear advantage is the homogeneity of our data, the same and consequent classification system, and the possibility of increasing data quality. The clear disadvantage is the missing comparability. The study’s retrospective nature is also a limiting factor in assessing trends. As trauma data cannot be presented prospectively, the study achieves the highest possible evidence level within its design limits. As our other study with the German Trauma Registry (DGU®) has shown, our centre data is statistically comparable with the data from Germany, Austria, and Switzerland and, therefore, represents an adequate sample of head and neck injuries. We assume that, in return, our data can also be extrapolated to the three above countries with an approximate inhabitant number of approximately 100 million [21].
The study timeline contains data before, during and after the COVID-19 pandemics. In our sample, the number of patients in the first pandemics year decreased 26% in comparison to 2019 and 20% in comparison to the average patient number in the years 2017–2019. This change fits to the literature, Alves et al. found 24% decrease in their review [22]. In international literature similar decrease was observed after implementing social distancing in 2020–2021. In the UK in this period, a clear change was found: the number of injured and the impact of the trauma decreased, the injury distribution has shown a different pattern [23]. Other demographic, epidemiologic or treatment factors were similar to those of our study [22,23,24,25,26]. There are much less data about post-pandemic epidemiology. We observed an increase in the number of patients nearly as high as in the pre-pandemic years. Similar is reported in literature [27].
The comparison of the two study groups showed significant differences. The isolated fracture group is in both genders younger than the panfacial group (6 and 3 years in males and in females respectively). Also, within study groups, males are much younger than females (16 and 13 years, respectively, in the isolated and panfacial groups). The male-to-female ratio is, however, very stable and comparable with literature data [8, 28,29,30].
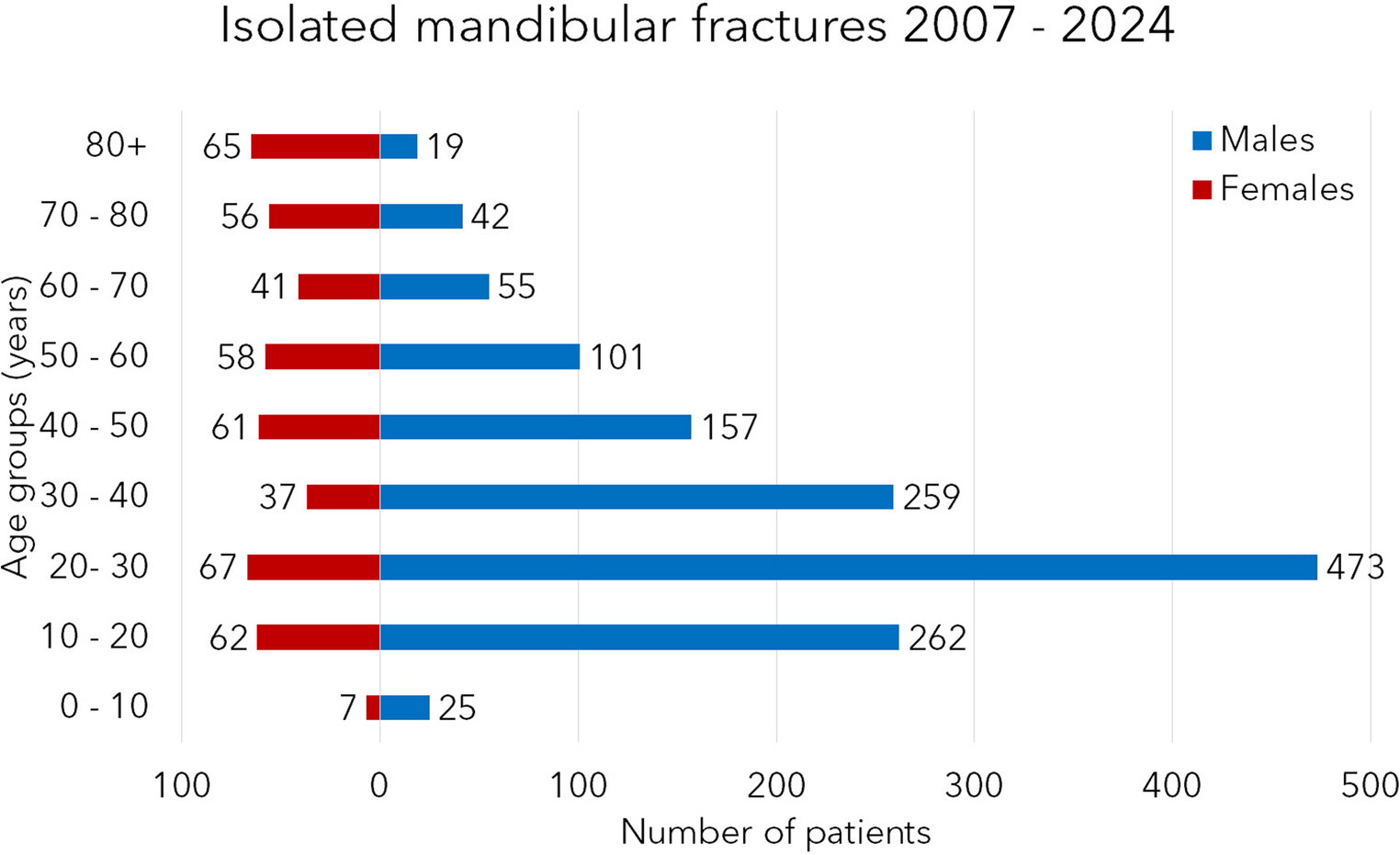
The age group distribution is very similar in the two groups. The most exposed are young males; the peak is in the age group of 20–30-year-olds. In females, the peak is smaller, and there is a double peak in the same age and in the age group of 80-year-olds and older. This second peak is much more marked in the panfacial group. As our previous studies and international papers stated, older females are a high-risk fracture group and a high-risk group for concomitant injuries [31, 32].
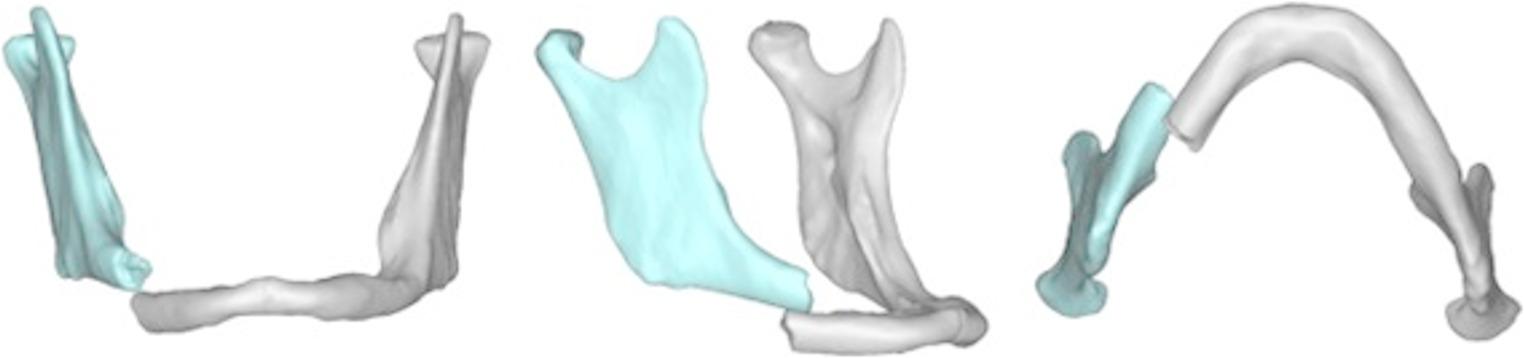
The fracture distribution in the mandibular area was statistically different between the two patient groups. Also, the visualization in Fig. 4 shows a more cranial distribution of the fracture sites. This can result from the different biomechanics of panfacial fractures (higher forces, other directions etc.). Similar distribution with an increased number of fractures of the articular process (and settlement of the most fractures to the cranial base or Frankfurt horizontal) was found in cases with concomitant cervical spine injuries both in our study and in the international literature [31,32,33,34,35]. Here, we must point out again that patients with panfacial fractures and older females with head and neck injuries are high-risk patients for suffering a concomitant cervical spine injury. Therefore, we suggest performing an initial CT scan of the complete head, cervical spine, and facial region. The different fracture distribution pattern should be taken into consideration during the first clinical examination, especially, if the patient is unconscious. The presented heatmap can warn all physicians working in the emergency department to exclude further injuries. It is very important to recognize fractures of the mandible near to the cranial base and to detect concomitant injuries to the auditory canal, cranial base or injuries to other cervical structures.
The fracture distribution in isolated cases is similar to those in the international literature [8, 29, 36,37,38,39,40]. In our study, 47% of the cases showed one fracture site, and in 53%, two or more, up to eight fractures. This means that if a fracture of the mandible was found, a second fracture should be excluded to be able to state the single fracture site.



Comments (0)