The aim of this study was to investigate potential risk factors, patient- and/or surgery-specific, for complications after orthognathic surgery based on data from NROK, a Swedish national patient register for orthognathic surgery. The results of the study showed that site of surgery, specifically interventions in the lower jaw and bimaxillary surgery, was clearly linked to postoperative complications after orthognathic surgery. Mandibular and bimaxillary procedures seems to increase the risk more than threefold for POI, removal of osteosynthesis material, and NSD, compared to maxillary surgery. For re-operation, there was no significant difference between the study groups. Other factors associated with the risk of postoperative complications were overweight, age over 40, smoking, and no postoperative antibiotics. Subgroup analysis of mandibular and bimaxillary surgery did not demonstrate any significant differences between the groups for the four postoperative complications reported.
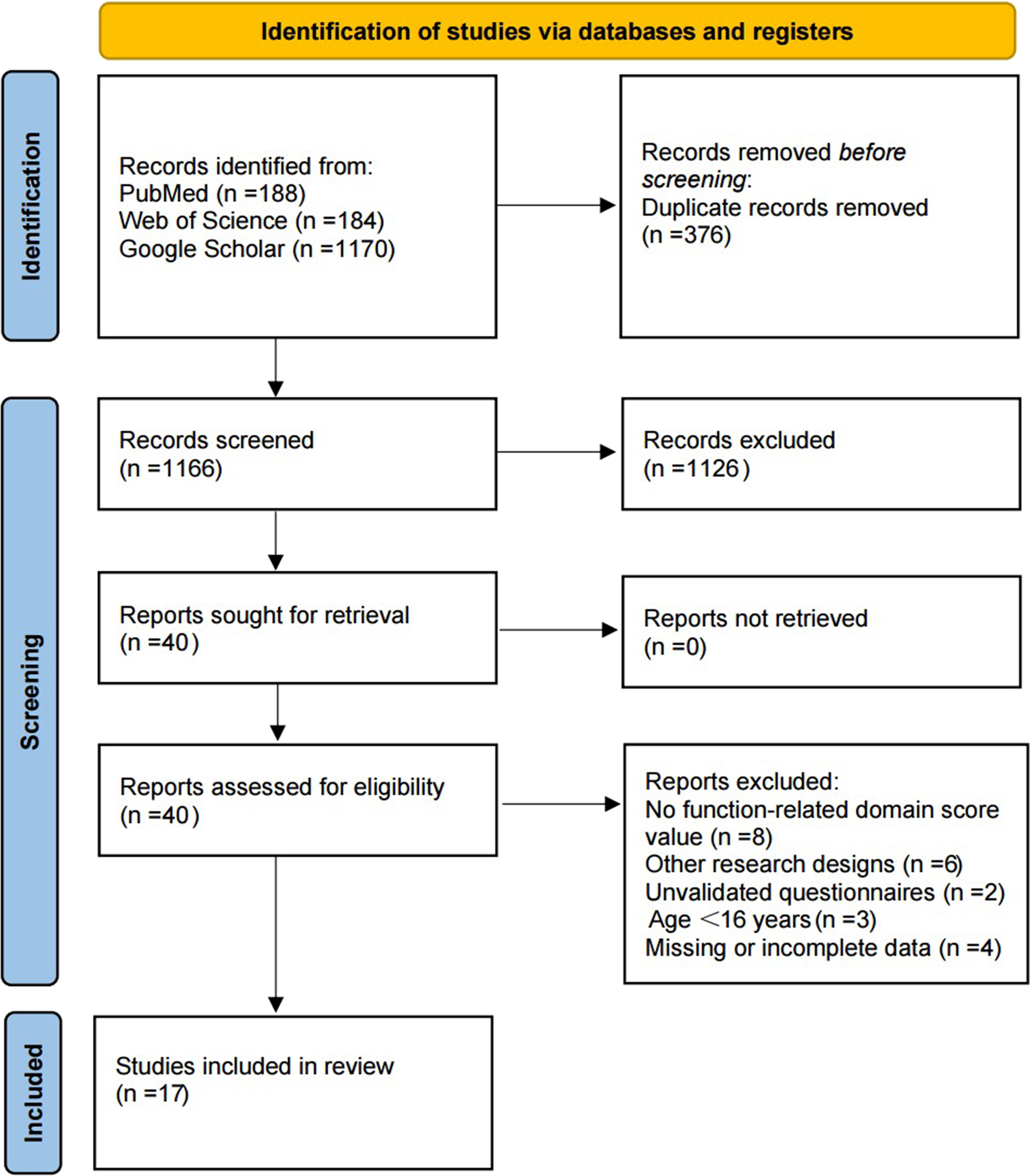
The dropout in the study signals the phenomenon of missing registration of the final examination 12-months postoperatively. Another factor that may have affected the dropout is the geographic mobility often characteristic for young people. It can be speculated that at the time of the final follow-up, not all operated patients were available for follow-up, as they could have moved from the region for work, educational purposes, or other reasons. In addition, a global COVID-19 pandemic broke out during the study period, with the possible consequence that not all patients were available for final follow-up. The potential confounding factors were dealt with using regression models. The main exposures appeared robust over the different models, yet unknown confounding factors may also be present in the material. One possible confounding factor could be the experience of the surgeons, which was not registered and is known to influence the outcome [20]. Selection bias might, however, be present, as the high overall dropout rate introduces a potential risk of bias in the results. A dropout analysis showed that the study population (428 patients) and the excluded group (543 patients) had a relatively similar distribution of background variables. This reduces the likelihood of a major impact on the outcome, suggesting that the results—despite a dropout rate of 55.9%—can be considered reasonably reliable.
Regarding information bias, one can consider how the data were measured and recorded in the different clinics. However, the definition and interpretation of the different parameters collected in NROK are defined in the online user manual for the register, which reduces information bias.
In total, the incidence of POI was 17%: 7% after SJmax, 20% after SJmand, and 21% after bimaxillary surgery. Other studies report an incidence of POI between 1% and 33% [5, 21,22,23]. An explanation for the fact that the incidence of POI was higher after SJmand and bimaxillary surgery could be that there is less vascularization in the mandible compared to the maxilla and therefore a vulnerability and an increase in the susceptibility to infection [24]. Another suggested explanation is that bacteria-rich saliva and food debris more easily accumulate along surgical incisions in the lower jaw, forming potential sources of postoperative surgical site infection (SSI) [2, 6, 25]. The risk of POI also increased significantly for patients with BMI < 25.5–30.0, as well as for underweight patients (BMI < 18.5), although this was not statistically significant for the underweight patients. Overweight is well-known to increase the risk of impaired wound healing and higher risk of SSI [26]. The risk for underweight people may be because the immune system is compromised due to nutritional deficiencies, which may affect wound healing and increase the risk of POI. Patients not receiving postoperative antibiotics had twice the risk of developing POI compared to those who received antibiotics. Davis et al. found that 25% of patients without postoperative antibiotics had SSI and only 4% of patients with postoperative antibiotic had SSI. BSSO was involved in 71% of the infections [21].
A systematic review by Naimi-Akbar et al., 2018, reported scientific uncertainties regarding the preferred antibiotic substance and optimal interval for prophylaxis in connection with orthognathic surgery [27].
Another systematic review by Blatt et al., 2019, showed that prolonged antibiotic regime for orthognathic surgery, may reduce the risk for surgical site infection, but there is a lack of evidence for the effects of short- vs. long-term therapy [28].
Presently, existing evidence has not shown that prolonged antibiotic prophylaxis beyond the day of surgery would provide a significant additional anti-infective effect against postoperative infection, but the risk of serious postoperative side effects and the development of antimicrobial resistance increases with prolonged prophylaxis [29]. Living in a larger city (≥ 50,000 inhabitants) was associated with higher risk (OR 2.484) of infection than those living in sparsely populated areas. One possible explanation could be that in more densely populated areas there is a higher risk of exposure to infection than in sparsely populated areas. Another possible explanation is that people living in sparsely populated areas have poorer access to healthcare and opportunity to seek care for postoperative infections, which would lead to underreporting of POI in sparsely populated areas. There are no previously published studies that explicitly address the difference in postoperative infections after orthognathic surgery between densely populated and sparsely populated areas.
Removal of osteosynthesis material was performed in 56 patients (13%) with significantly higher risk after SJmand and bimaxillary surgery than after SJmax. Other studies reported plate removal after orthognathic surgery from 2.8% to 27.5% [11, 23, 25, 30,31,32,33,34,35]. In previous published studies, smoking [22, 32], increasing age [31, 33], operations performed in the mandible [32], and length of operation [33] are described as risk factors for plate removal. A total of 32 patients underwent re-operation (7.5%). No significant difference was noted between the groups. For smokers and patients 40–75 years of age, the risk of re-operation increased significantly.
Smoking affects the body both at a molecular and cellular level, including peripheral vasoconstriction and tissue hypoxia, which can lead to impaired wound healing and an increased risk of POI [22, 26, 36,37,38]. However, the number of smokers in the current study population was relatively small, so the results should be interpreted with caution. The overall rate of re-operation in this study agrees with previously published results [9, 12, 39].
The incidence of NSD 12 months postoperatively was 33%: 15% after SJmax, 35% after SJmand, and in 40% after bimaxillary surgery. Female gender and no postoperative antibiotics significantly increased the risk of NSD. Kuhlefelt et al. identified increasing age, large mandibular displacements, manipulation of the inferior alveolar nerve, and large jaw angle as predisposing to neurosensory disturbance [40]. According to Blomqvist et al., [41] older patients are more often affected by NSD after BSSO than younger patients with similar conditions. Yoshioka et al. [42], reported gender differences for NSD (women 78% vs. men 22%) after BSSO, which the authors explained by anatomical differences in the location of the nerve canal and the hardness of the bone.
The strengths of this register-based study are related to the data registered and obtained from NROK, a national register with good geographic coverage, which increases the external validation of the results. A weakness is that NROK is a new register, launched in 2017, as it may take time to incorporate data registration as part of the clinical routine. Compliance to register data seems to be especially challenging at last follow-up visit. However, important strengths of the study are the size of the study population and registration from multiple clinics contributing to a low risk of random variation. This study is new in its kind based on data from a national orthognathic register.
Given that the NROK register is new, it would be valuable to repeat this study with the same aim and hypothesis, to compare data collected over a longer period, with more robust data, and with less dropouts.



Comments (0)