Selection of first-line agents to treat patients with advanced NSCLC and atypical EGFR mutations must balance efficacy with toxicity. In phase 3 trials, osimertinib monotherapy has demonstrated clinical efficacy and favorable safety in previously untreated patients with EGFR-mutated (Ex19del or exon 21 L858R substitution, with or without T790M) advanced NSCLC [9, 10, 14]. Consequently, osimertinib is recommended as a first-line treatment option for patients with advanced NSCLC and classical sensitizing EGFR mutations [15,16,17,18]. While osimertinib is also recommended, alongside afatinib, as a front-line treatment option for patients with advanced NSCLC and atypical EGFR mutations [15], these recommendations are based on limited data [19, 31], reflecting the relatively low prevalence of atypical EGFR mutations [5]. With the paucity of available data, understanding outcomes with first-line osimertinib monotherapy in patients with atypical EGFR mutations in routine clinical practice is critical.
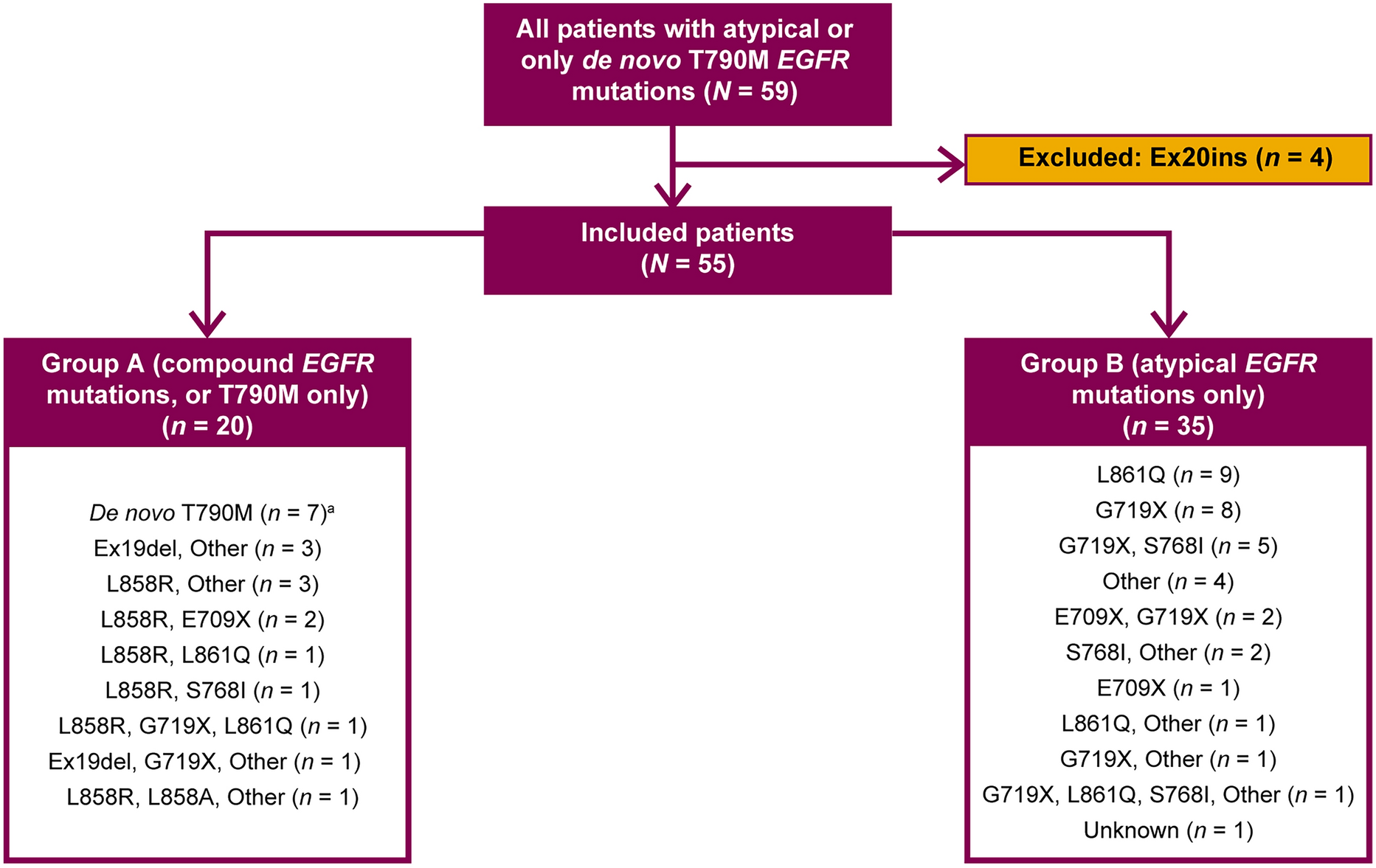
Despite the limited patient numbers, this study is one of the largest USA-wide, real-world studies conducted to date describing outcomes with first-line osimertinib and subsequent treatment patterns in patients with advanced NSCLC and atypical EGFR mutations. A total of 55 patients were included in the analyses, of whom 35 had tumors harboring atypical EGFR mutations only and 20 had tumors harboring compound EGFR mutations or de novo T790M mutations only. Notably, the demographics and baseline characteristics of these patients were broadly consistent with those reported previously in other observational studies of patients with atypical EGFR mutations [20, 22, 27, 28, 32]. Of note, while the high rate of smoking history (69%) in patients with atypical EGFR mutations is consistent with that reported in other studies (reported rates, 52–81%) [19, 21, 22, 27, 32], it is higher than that observed in patients with classical EGFR mutations, with rates of 44–45% reported from such patients using similar data extracted from the Flatiron database [33, 34]. This observation underscores the importance of broad-based genomic testing, irrespective of smoking history. Among all 55 patients, median TTNTD was 12.8 months and median TTD was 10.7 months, while estimates of median rwPFS and median OS were 8.8 and 28.5 months, respectively. As also seen for other EGFR-TKIs and in other studies of osimertinib [21, 23, 27, 32], survival outcomes in the present study, including both rwPFS and OS, were longer in patients with compound EGFR mutations or de novo T790M only than in those with atypical EGFR mutations only (median rwPFS, 20.3 vs. 6.6 months, respectively; median OS, 42.5 vs. 20.0 months, respectively). However, the data should be interpreted with caution, given that no formal analysis was conducted, patient numbers are limited, and the 95% CIs for the median estimates are wide. In vitro data have consistently shown greater cell killing with osimertinib when the classical L858R substitution and atypical E709K mutation are both present compared with the presence of a single E709K mutation [3]. Our data, which suggest trends for better outcomes in patients with compound EGFR mutations or de novo T790M mutations only than in those with atypical EGFR mutations only, are consistent with these findings.
Although previous studies have suggested that patients with tumors harboring T790M mutations may be more responsive to first-line osimertinib than those without these mutations [21, 35, 36], the sensitivity analysis from the current study showed similar estimates for OS in patients with compound EGFR mutations irrespective of the inclusion or exclusion of patients with de novo T790M mutations only. However, as just seven patients (13%) had de novo T790M mutations only, the limited sample size makes this result difficult to interpret. It is also possible that these patients may have harbored mutations not captured in the database.
Importantly, our estimates of real-world outcomes with osimertinib monotherapy in patients with advanced NSCLC and atypical EGFR mutations only are similar to those reported previously in the literature [19,20,21,22,23, 27, 28, 32], including phase 2 non-randomized studies conducted in Korea (n = 36; median PFS 8.2 months, median OS not reached), the USA (n = 17; median PFS 10.5 months, median OS 13.8 months), and Japan (n = 40; median PFS 9.4 months, median OS not reached); a post hoc subgroup pooled analysis from two phase 2 studies conducted in Northern Europe (n = 21; median PFS 5.5 months, median OS 11.9 months); and observational studies conducted in Europe (UNICORN n = 44; median PFS 8.6 months, median OS 22.1 months), the USA (n = 36; median PFS 11.7 months, median OS 26 months), and Italy (ARTICUNO; n = 66; median PFS 8 months, median OS 17 months). The consistency of outcomes from these relatively large real-world studies with our findings from US patients suggests that our results may be generalizable with a more global patient population.
Our results are also similar to those reported for afatinib, another first-line treatment option in this setting [15, 16], in a post-hoc analysis of patients with EGFR-TKI-naïve, advanced NSCLC harboring atypical EGFR mutations who received afatinib within the context of the LUX-Lung trials [31]. Among 38 patients with tumors harboring point mutations or duplications in exons 18–21 (excluding T790M), median PFS was 10.7 (95% CI 5.6–14.7) months and median OS was 19.4 (95% CI 16.4–26.9) months [31].
A recent systematic review of objective responses to EGFR-TKIs in patients with advanced NSCLC harboring atypical EGFR mutations has indicated that afatinib may be the most clinically active treatment for patients with tumors harboring S768I, G719X, E709X, and L747X mutations, whereas osimertinib appears to be most active in patients with tumors harboring an L861Q mutation [37]. Our results indicate that first-line osimertinib monotherapy provides some degree of clinical benefit for patients with NSCLC harboring various atypical EGFR mutations, but the subgroups are too small to infer meaningful differences across the mutation types, as was also the case in the UNICORN study [21].
Among all 55 patients in the present analysis, by the end of follow-up, 13% remained on first-line osimertinib monotherapy and 33% went on to receive second-line treatment (most commonly osimertinib combinations, chemotherapy, immunotherapy, or other EGFR-TKIs [including osimertinib]). Notably, more than half of the 55 patients (54%) did not receive second-line treatment due to death; optimizing first-line treatment through combining osimertinib with chemotherapy, which has been shown to improve PFS compared with osimertinib monotherapy in patients with NSCLC harboring predominantly classical EGFR mutations [14], might have benefited these patients. The proportion of patients who remained on first-line osimertinib was lower in patients with atypical EGFR mutations alone than in those with tumors harboring compound EGFR mutations or de novo T790M mutations only, which may reflect the lower effectiveness of EGFR-TKIs in this subpopulation [5], along with the lack of consistent guidelines for these patients. However, the proportion of patients who went on to receive second-line treatment was similar in both subgroups. Disease progression was the most common reason for osimertinib discontinuation in both subgroups, with a higher proportion of patients with tumors harboring atypical EGFR mutations only discontinuing treatment for this reason than those with tumors harboring compound EGFR mutations or de novo T790M mutations only, again likely mirroring the reduced effectiveness of EGFR-TKIs in patients with NSCLC harboring atypical EGFR mutations [5]. To our knowledge, this is the first report of real-world subsequent treatment patterns following first-line osimertinib in patients with advanced NSCLC and atypical EGFR mutations.
This analysis is subject to the limitations typically associated with retrospective, observational database studies, such as potential measurement errors, inconsistent data quality, missing data, and coding errors and variability. There were also no data available on the races categorized as “Other,” the objective response to treatment, CNS efficacy, or tolerability of treatment (which were major limitations of the study). An analysis by sex/gender was not conducted due to low patient numbers; however, given that previous clinical trials of EGFR-mutated advanced NSCLC have shown similar efficacy for osimertinib irrespective of patient sex/gender [9, 10, 14], it is unlikely that such an analysis would have affected interpretation of the results. Due to the lack of formal comparative analyses, it was not possible to derive conclusions on the comparative effectiveness of osimertinib treatment in the two subgroups, among different mutation types, or relative to alternative treatments, such as afatinib. Because the Flatiron Health data are obtained mainly from community oncology settings, assessment of progression may have varied across centers and some patients may have progressed before the date of their recorded progression. However, as the TTNTD and TTD measures supported the rwPFS data, any recording errors are unlikely to have had a major impact on the results. Furthermore, potential biases may have been introduced by differing data capture frequency in community settings. As stated above, this is a relatively large real-world study reporting outcomes for first-line osimertinib in patients with advanced NSCLC harboring atypical EGFR mutations in comparison with previous reports, yet the sample sizes were small, especially in the subgroups; therefore, these results should be interpreted with caution. Nonetheless, the similarity of the baseline characteristics and outcomes observed in our patient population compared with previous reports [19,20,21,22,23, 27, 28, 32] suggest that the findings are representative of patients with advanced NSCLC and atypical EGFR mutations.



Comments (0)