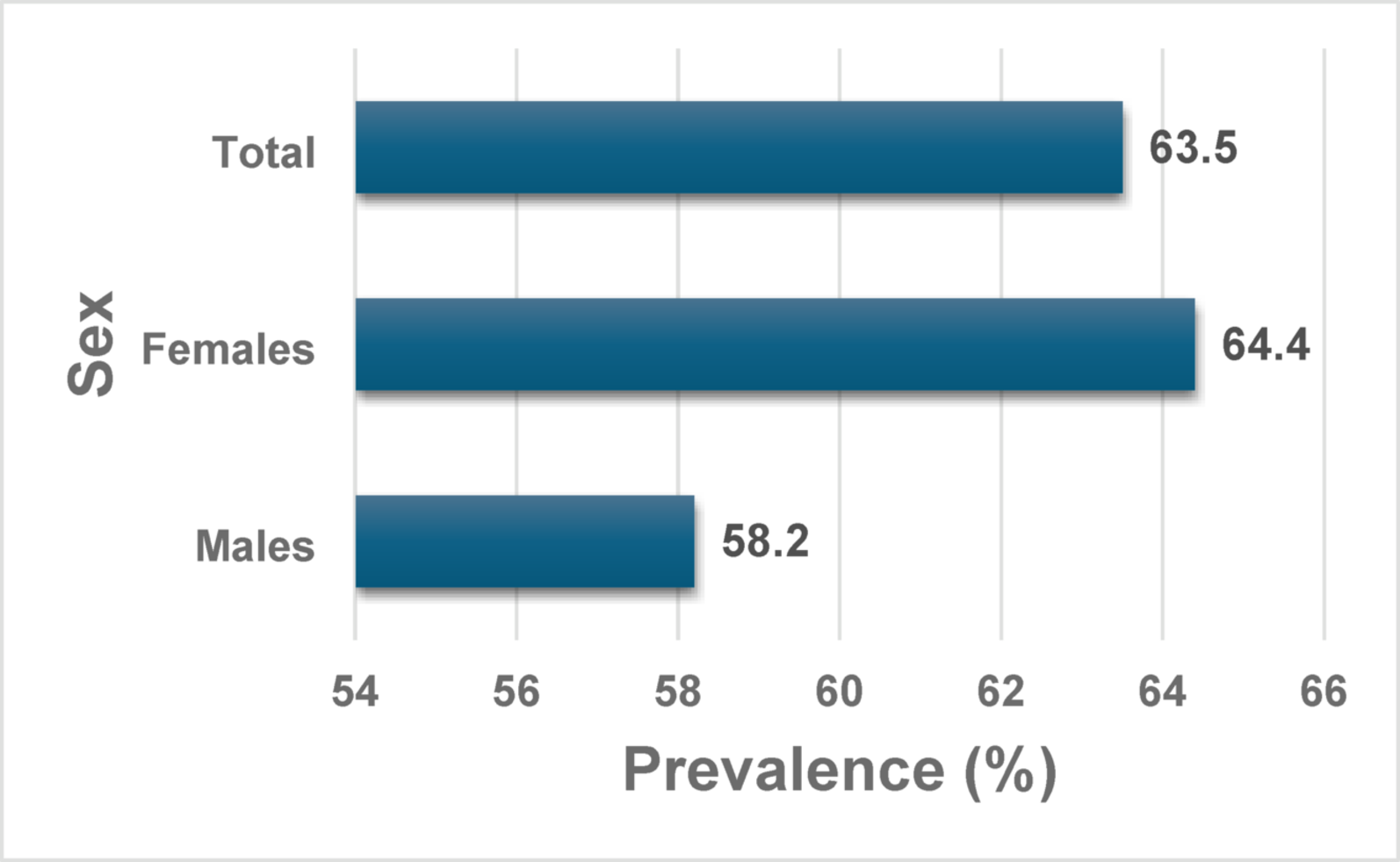
This study reveals a high dyslipidemia prevalence of 64.1% among people living with HIV (PLHIV) in Ghana’s Eastern Region, a finding that underscores a significant and pressing public health challenge. This high burden is consistent with the well-documented shift in morbidity and mortality among PLHIV, from AIDS-defining illnesses to non-communicable diseases like cardiovascular disease (CVD). Our prevalence is situated within the wide spectrum reported across sub-Saharan Africa; it is lower than the 78% observed in a Ugandan cohort on dolutegravir-based ART but substantially higher than the 28% found in a study from Western Ghana and the 51.1% (low HDL-C) in Nigeria [1, 5, 8]. These regional disparities are likely multifactorial, stemming from differences in ART regimens (as newer integrase inhibitors may have distinct metabolic effects), population demographics, genetic predispositions, underlying lifestyle factors, and the specific diagnostic criteria used. Our study also identified a higher prevalence among females (64.4%) compared to males (58.2%), a gender disparity seen in other African studies [9, 10]. This may be attributable to complex interactions between hormonal influences on lipid metabolism, gendered social roles affecting diet and physical activity, and potential sex-specific responses to ART. Regardless of the precise comparison points, the conclusion is clear: dyslipidemia represents a major co-morbidity in the Ghanaian HIV-positive population, necessitating the urgent integration of CVD risk assessment and management into routine HIV care.
A central finding of our analysis is that the primary drivers of dyslipidemia in this cohort were modifiable lifestyle and body composition factors, rather than ART-related variables or core demographics. Specifically, after adjusting for confounders, individuals who consumed alcohol had more than double the odds of having dyslipidemia (aOR = 2.05, 95% CI: 1.20–3.52), and those who were physically inactive had nearly double the odds (aOR = 1.88, 95% CI: 1.12–3.15). These strong associations align with established evidence linking these behaviors to adverse metabolic profiles through mechanisms such as increased hepatic triglyceride synthesis from alcohol and reduced lipid catabolism from inactivity [4, 14]. Furthermore, our data highlight the critical importance of body composition. Every one-unit increase in Body Mass Index (BMI) was associated with a 24% increase in the odds of dyslipidemia (aOR = 1.24, 95% CI: 1.02–1.50). More notably, increased muscle mass was found to be significantly protective, with each unit increase associated with a 15% reduction in the odds of dyslipidemia (aOR = 0.85, 95% CI: 0.75–0.97). This latter finding suggests that clinical interventions should not only focus on reducing overall adiposity but must also prioritize the preservation and building of lean body mass, a crucial factor often overlooked in weight management programs. This is particularly relevant in the context of HIV, where chronic inflammation can contribute to sarcopenia. These results collectively point to a clear and actionable conclusion: lifestyle interventions that promote physical activity (including resistance training), support healthy weight management, and encourage reduced alcohol intake are critical and powerful tools for mitigating dyslipidemia risk in this population.
Our analysis also produced unexpected results that warrant careful interpretation and further investigation. Most notably, a history of ever smoking appeared to be protective against dyslipidemia (aOR = 0.16, 95% CI: 0.06–0.41). This counterintuitive finding starkly contradicts the vast body of evidence that firmly establishes smoking as a major risk factor for atherogenic dyslipidemia and CVD [9, 10]. This paradox is likely a reflection of our study’s limitations. The low prevalence of smoking within our predominantly female cohort (85%) may have provided insufficient statistical power to detect the true, harmful effect. Moreover, our cross-sectional design is susceptible to survival bias, where smokers who developed severe dyslipidemia and subsequent cardiovascular events may have been less likely to survive and be included in the study sample. Finally, the use of a simple “ever smoked” metric is a crude measure that cannot capture the dose-dependent and duration-dependent risks of tobacco use. We also found no significant association between dyslipidemia and ART regimen/duration, age, or education level. While numerous studies have identified these as key determinants [11,12,13], their effects in our cohort may have been overshadowed by the profound influence of the lifestyle and body composition factors discussed above. The relative homogeneity of our sample’s treatment (predominantly TDF-based first-line ART) and demographics could also have attenuated these associations.
This study has several limitations that must be acknowledged. Its cross-sectional design precludes the establishment of causal relationships between the identified risk factors and dyslipidemia. The logistic regression model explained 20.4% of the variance in dyslipidemia status (Nagelkerke R²), which, while statistically significant, indicates that nearly 80% of the risk is attributable to unmeasured factors. These likely include specific ART agents not analyzed in detail, genetic predispositions to metabolic disorders, which are known to vary in African populations [14], and more detailed dietary patterns beyond a simple diversity score (e.g., intake of saturated fats, trans fats, and sugars). Furthermore, the lack of data on biomarkers of systemic inflammation (e.g., hs-CRP, IL-6) or detailed HIV disease history (e.g., CD4 nadir, duration of viral suppression) prevents a deeper exploration of the immunological pathways influencing lipid metabolism. Finally, the study was conducted in two facilities within one region of Ghana and included a predominantly female sample, which may limit the generalizability of our findings to other populations.



Comments (0)