
Remember me


On November 25th 2022, a 28-year-old homosexual male from Indonesia, who had been living in Germany for over four years, was diagnosed with advanced HIV/AIDS during outpatient evaluation for symptoms of dyspnea and the microbiological confirmation of Pneumocystis jirovecii pneumonia (PCP) and esophageal candidiasis. Laboratory results revealed profound immunosuppression with a CD4 + T-cell count: 4 cells/µL; CD4/CD8 ratio: 0.89; HIV viral load: 2,010,000 copies/mL, consistent with CDC Stage C3 disease [2]. He was started on high-dose intravenous trimethoprim-sulfamethoxazole for PCP, fluconazole for esophageal candidiasis, and after two more weeks started on antiretroviral therapy (ART) with a fixed-dose combination of bictegravir, emtricitabine, and tenofovir alafenamide.
On December 21st, 2022, two weeks after initiating ART, the patient was transferred to our hospital due to rapid clinical deterioration. Laboratory findings at that time revealed a paradoxical response: despite a profound immunological recovery with his CD4 + T-cell count increasing from 4 to 421 cells/µL, his HIV viral load had not suppressed and was measured at 472,000 copies/mL (Fig. 1). This was accompanied by worsening symptoms including persistent fever, weight loss, and abdominal discomfort, which led to his transfer to the intensive care unit (ICU) for progressive dyspnea and acute respiratory failure. At ICU admission, he showed severe wasting (BMI: 15.9), pancytopenia, and required mechanical ventilation.
The combination of rapid immune recovery under ART, followed by a rapid clinical decline and a decreasing CD4 + T-cell count, strongly suggested the development of severe immune reconstitution inflammatory syndrome (IRIS). Considering the life-threatening respiratory failure and critical condition, the team made the decision to pause ART to mitigate further immune activation in the context of life-threatening hyperinflammation. While discontinuation of ART is generally not recommended, current guidelines allow for interruption in exceptional cases where corticosteroids fail to achieve improvement [3].
Given the patient’s origin from an endemic region, the miliary radiological pattern, and systemic deterioration despite ongoing treatment with high-dose trimethoprim-sulfamethoxazole and fluconazole, disseminated histoplasmosis was considered early as a likely underlying cause of IRIS and empiric antifungal therapy was initiated.
Bronchoalveolar lavage fluid (BALF) obtained on admission revealed Pneumocystis jirovecii, cytomegalovirus (CMV), and Pseudomonas aeruginosa. In response, antimicrobial therapy was escalated to include piperacillin/tazobactam at 4.5 g every six hours, doxycycline at 100 mg twice daily, empiric amphotericin B at 0.7 mg/kg daily for the suspected IRIS-trigger and ganciclovir at 5 mg/kg twice daily. Although histopathologic confirmation of CMV pneumonitis was not available, PCR positivity in BALF, the patient’s critical immunosuppression, and the anticipated use of further immunosuppressive agents led to the precautionary initiation of antiviral therapy. Methylprednisolone was administered at 500 mg/day for three days but failed to improve respiratory or hemodynamic status.
The patient remained critically ill, requiring high inspired oxygen fractions (FiO₂ up to 0.84) and vasopressor support. Laboratory and imaging findings at that time fulfilled with five out of eight of the HLH-2004 criteria [4]: persistent fever, hepatosplenomegaly, pancytopenia, hypofibrinogenemia of 0.9 g/L (< 1.5 g/L) and markedly elevated ferritin concentrations of 138,740 µg/L (>100,000 µg/L).
Due to steroid-refractory IRIS/HLH and progressive clinical deterioration, immunosuppressive therapy was escalated. The patient received intravenous immunoglobulin (IVIG, 400 mg/kg/day), the interleukin-1 receptor antagonist anakinra (100 mg daily), the Janus kinase (JAK) inhibitor ruxolitinib (5 mg twice daily for a total of 16 days), and cytokine adsorption therapy using a CytoSorb® filter integrated into a continuous renal replacement therapy (CRRT) circuit for a duration of five days [5].
Bone marrow aspirates ruled out mycobacterial and leishmanial infections and revealed no signs of hemophagocytes. Given the clinical and radiographic overlap with tuberculosis and the patient’s origin from an endemic region, disseminated histoplasmosis was considered [6]. The diagnosis of disseminated histoplasmosis was robustly confirmed on December 31, 2022, through a multi-modal approach performed by the German National Reference Center for Histoplasmosis at the Robert Koch Institute. This included both a positive antigen test and a positive PCR from serum and BALF, providing strong evidence from different methodologies. The diagnosis was further solidified by an additional positive 18 S-PCR from a bone marrow sample, confirming systemic involvement [7].
The patient gradually improved under combined antifungal treatment (liposomal amphotericin B until January 19, 2023, followed by itraconazole) and intensified immunosuppression. The patient’s co-infections with Pneumocystis jirovecii, CMV, and Pseudomonas aeruginosa were successfully managed, as evidenced by a decline in inflammatory markers like C-reactive protein, negative follow-up blood cultures, and sustained clinical improvement. Due to persisting anemia, ganciclovir switched to prophylactic dose after 21 days of therapeutic dosing with a subsequent increase in hemoglobin. However, briefly afterwards, the patient reported bilateral vision loss and ophthalmological examination revealed suspected bilateral CMV retinitis, which was supported by rising number of CMV copies in blood. CMV-retinitis was successfully managed with oral valganciclovir – a re-decrease of hemoglobin was to be tolerated – and laser treatment. On January 10, 2023, ART was reinitiated using a protease-inhibitor–based regimen comprising darunavir, ritonavir, and dolutegravir. Viral suppression and immune recovery were evident, with the CD4 + T-cell count rising to 485 cells/µL by January 19th. Respiratory function improved steadily, follow-up imaging demonstrated resolution of pulmonary infiltrates, and the patient was discharged in stable condition, eventually returning to work.
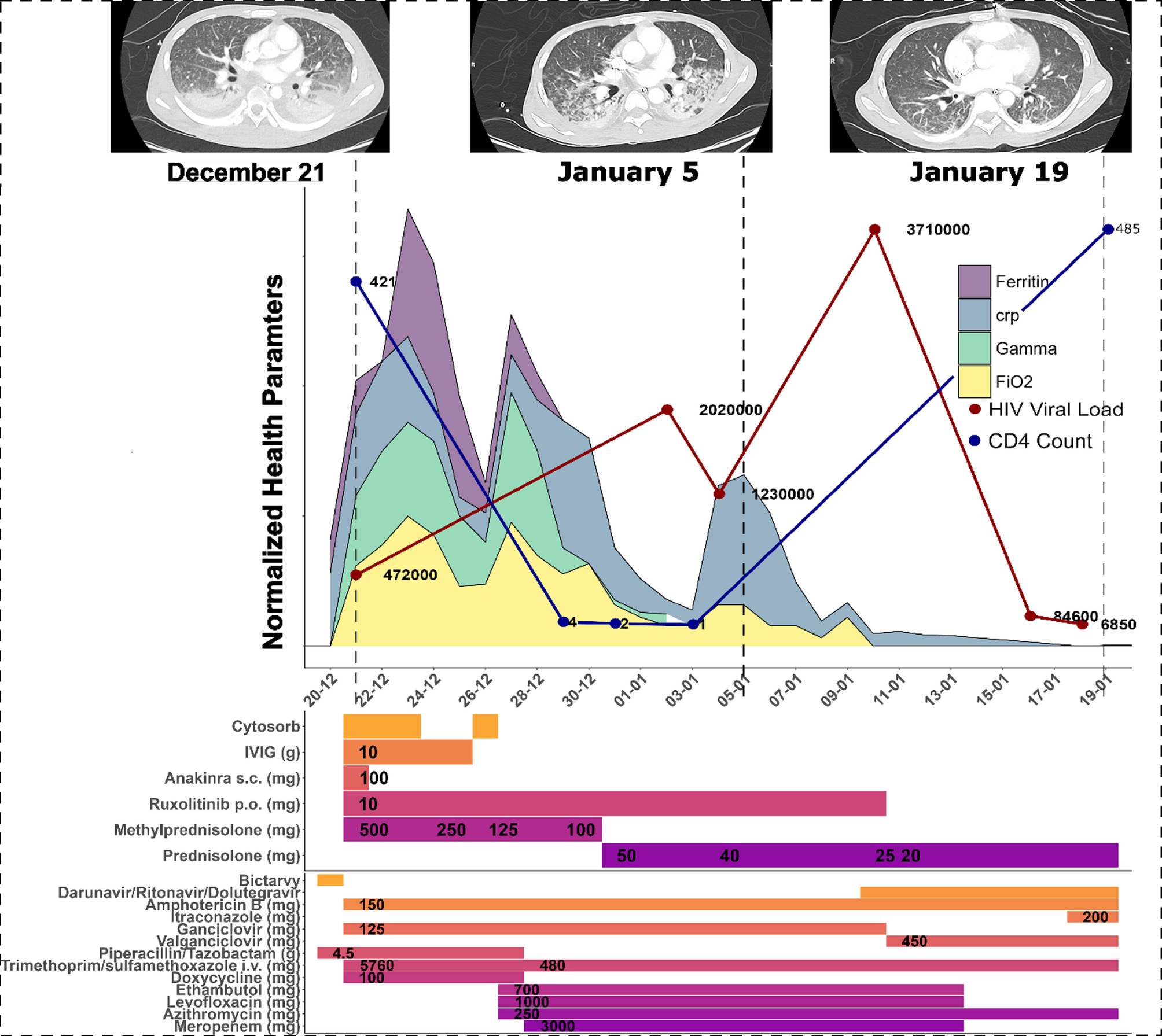
Fig. 1
Clinical and Therapeutic Timeline: The figure illustrates the patient’s clinical course and treatment from December 21, 2022, to January 19, 2023. The main panel shows density plots with normalized trajectories of key inflammatory and clinical parameters, including Ferritin, C-reactive protein (CRP), norepinephrine requirement (Gamma), and the fraction of inspired oxygen (FiO2). Overlaid on this graph are the specific data points for the patient’s HIV viral load (red dots) and CD4 + T-cell count (blue dots), with their corresponding values labeled. The middle panel details the timeline and dosages of administered immunosuppressive therapies, including cytokine adsorption (CytoSorb®), intravenous immunoglobulins (IVIG), Anakinra, Ruxolitinib, Methylprednisolone, and Prednisolone. The bottom panel presents the timeline and dosages of anti-infective and antiretroviral therapies
Comments (0)