
Remember me


We reviewed national guidelines from the following eight countries: Ethiopia, Ghana, Ivory Coast, Mozambique, Republic of Congo, Rwanda, Tanzania, and Zambia [13,14,15,16,17,18,19,20]. Six had a specific section for AHD. Guidelines were published between 2019 and 2023.
Information extracted from national guidelines is presented in Table 1 and agreement with the WHO 2021 document in Table 2. The index of assessed guidelines is shown in Table 3.
Table 1 Extracted data country specific guidelinesTable 2 Agreement of country specific guidelines to WHO 2021Table 3 Index of national guidelinesDefinition of AHDThe Ivory Coast guideline did not include a definition of AHD. All other national guidelines employed the same definition as the WHO, considering a CD4 + cell count < 200 cells/mm3 or a WHO clinical stage 3 or 4 disease as AHD.
ScreeningCD4 testingAll national guidelines recommended CD4 count testing for people with HIV (PWH) entering or re-entering antiretroviral therapy (ART) care, which is in line with the WHO 2021 recommendations. However, the Republic of Congo recommended performing CD4 testing only for those in whom ART is started.
Cryptococcal diseaseExcept of Ivory Coast, all guidelines recommended serum cryptococcal antigen testing, but there were differences in the population to be tested, resulting in partial agreement for the documents of Mozambique, Tanzania, and Zambia. Based on the WHO guideline (recommended < 100 cells/mm3, considered: < 200 CD4 + cells/mm3) we counted < 100 cells/mm3 as agreement and < 200 CD4 + cells/mm3 as partial agreement. Tanzania and Zambia guidelines recommended testing for CD4 + < / ≤ 200 cells/mm3. The Mozambique guidelines recommended testing if additional criteria are met, including danger signs or suspicion of cryptococcal disease, or WHO stage 3 or 4 disease.
TuberculosisIn line with the WHO, all national guidelines recommended screening for TB. The use of urine lipoarabinomannan (LAM) testing to screen for tuberculosis was discussed in all national guidelines except those from Ivory Coast. Only the Ghanaian and Ethiopian guidelines separated the targeted population by in- and out-patient as per WHO 2021 guidance (inpatient: ≤ 200 cells/mm3, outpatient ≤ 100 cells/mm3, or any CD4 count with symptoms or if seriously ill). All guidelines recommended the use of urine LAM in patients who are severely ill or have danger signs, independently of CD4 count.
Prophylaxis for opportunistic infectionsCotrimoxazoleAll national guidelines recommended cotrimoxazole (CTX) prophylaxis but there were differences in the criteria for timing of initiation and discontinuation. According to the WHO 2021 guidance, CTX should be provided to all PHW with a CD4 cell count of less than 350 cells/mm3 or clinical stage 3 or 4 disease, or in settings with high prevalence of malaria or severe bacterial infection. The Zambian guidelines recommended starting CTX if the CD4 counts is < 350 cells/mm3 or with clinical stage 3 or 4 disease. Ivory Coast and Republic of Congo guidelines recommended starting CTX in all PWH irrespective of the CD4 count, based on the high prevalence of malaria or severe bacterial infections. Mozambique guidelines expanded the use of CTX to also include patients with WHO clinical stage 2. Ethiopia, Ghana, Tanzania, and Rwanda guidelines recommended CTX for all PWH with active tuberculosis regardless the level of CD4, with differences in other indications. Except the use of CTX in patients with tuberculosis, guidelines of Ghana recommended CTX in line with the WHO 2021; Rwanda guidelines considered virologic failure (HIV RNA > 200 copies/ml) as a criterion for treatment; Ethiopian and Tanzania guidelines did not provide additional clinical criteria for initiating CTX prophylaxis.
All guidelines except those from Rwanda provided guidance for discontinuation of CTX for PWH. The WHO 2021 stated that CTX can be stopped if a patient is stable on ART with immune recovery or viral suppression. Guidelines from Ghana, and Tanzania aligned with the WHO guidance. In settings with a high burden of malaria or severe bacterial infections, CTX should be continued regardless of CD4 count or clinical stage, which is recommended in the guidelines of the Republic of Congo. Ethiopian guidelines include an option to discontinue prophylaxis with combining HIV viral load testing and CD4 testing. All other national guidelines recommended discontinuing CTX prophylaxis based on CD4 counts.
Cryptococcal antigenemia and tuberculosis preventive therapyOther than the guideline of Ivory Coast, which do not address this item, all guidelines recommended pre-emptive therapy for cryptococcal antigenemia. All national guidelines recommended tuberculosis preventive therapy for all PWH.
Supportive care interventionsThe Guidelines of Ivory Coast and Tanzania did not provide any information about supportive care interventions. Recommendations for adherence for people with AHD from the other countries included measures such as home visits or specific communications interventions.
Antiretroviral therapyRegimenThe recommended first-line ART regimen for all countries was in line with the WHO guideline: Dolutegravir (DTG)/ lamivudine (3TC)/ tenofovir disoproxil fumarate (TDF) or DTG/emtricitabine (FTC)/TDF.
Timing of ART initiation in the presence of opportunistic infectionsNon-neurological TBThe WHO guidelines recommend starting ART within 2 weeks for PWH with tuberculosis at a non-neurological site, independent of CD4 cell count. Guidelines from Ethiopia, the Republic of Congo, Mozambique, and Tanzania provided the same recommendation; Zambian guidelines recommend a start within ten days. Ivory Coast guidelines recommended deferring ART initiation for 2 weeks. Rwandan guidelines took a similar approach but suggested starting ART within 4–6 weeks for CD4 counts above 50 cells/mm3. Ghana guidelines recommended to start ART as soon as possible and within two weeks if practicable but latest after 8 weeks and initiation should be deferred if clinical symptoms suggest meningitis.
Tuberculous meningitis (TBM)WHO 2021 guidelines recommend delaying start of ART for 4–8 weeks for patients with TBM. Ethiopian guidelines provided the same information. Guidelines from Ghana, and Mozambique recommended slightly different timings for ART initiation, but were similar to WHO recommendations. The guideline of Ivory Coast would start as early as 4 weeks, Rwanda and Zambia within 4–6 weeks. The guidelines of the Republic of Congo did not specify any timing. Tanzania guideline stated to start ART as soon as possible and within 2 weeks after TB treatment.
Cryptococcal meningitisGuidelines from Ethiopia, Ghana, Mozambique, and Rwanda recommended deferring start of ART for 4–6 weeks for people with cryptococcal disease, which is consistent with the WHO 2021 guidelines. Tanzania’s guideline recommended deferral for 5 weeks (considered as agreement). The Zambian guideline recommended deferral of ART but do not specify any time period. The Republic of Congo guideline did not provide a clear timeline and the guideline from Ivory Coast did not address this issue.
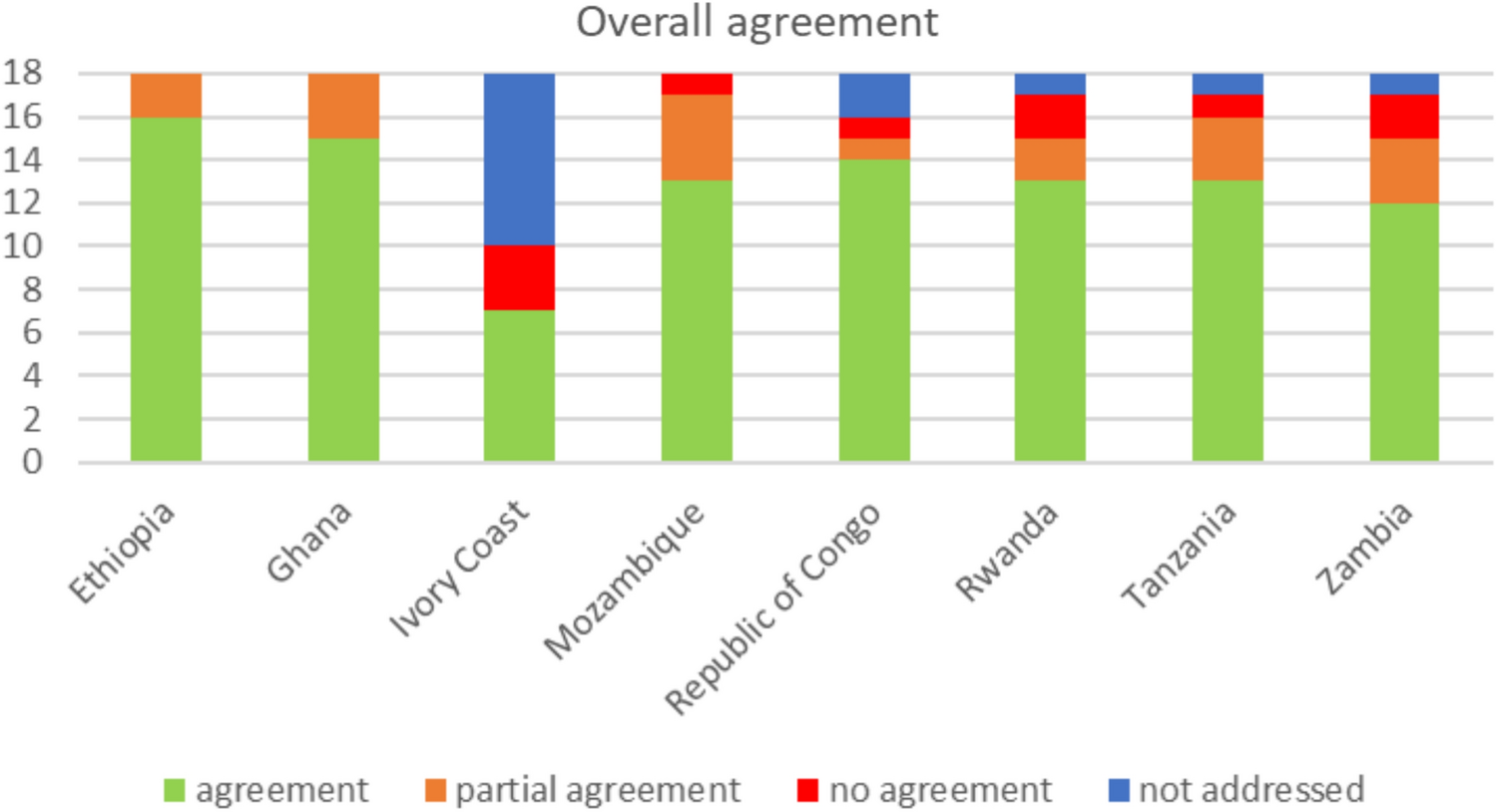
Overall agreementOverall agreement for all assessed items (total 18) ranged from 7.0 for the Ivory Coast guideline to 17.0 for the guidelines from Ethiopia (Fig. 1). None of the national guidelines had more than three items not in agreement with the WHO guidelines, and the maximum number of items not addressed by any one guideline was eight. Except the guideline of Ivory Coast (overall agreement: 7.0), all documents showed similar overall agreement (range: 13.5–17.0), irrespectively of publication date (Fig. 2).
Fig. 1
Overall agreement by country
Fig. 2
Overall agreement according to year of publication
Comments (0)