
Remember me




Twenty-one patients with extracerebral AVMs (9 males, 12 females) underwent a total of 31 BEST/BEET procedures (Supplemental Table 1). Seventeen (81.0%) patients were part of the prospective multicenter study APOLLON; four (19.0%) patients were ineligible due to age limitation (≤ 4 years) but received similarly structured follow-up. The median age was 33 years (range, 0.5–53 years) at treatment. Twelve (57.1%) AVMs involved the face, with 5/21 (23.8%) lesions including lips (Fig. 1 and Supplemental Fig. 1), 4/21 (19.0%) enoral areas, and 1/21 (4.8%) periorbital region. Furthermore, 7/21 (33.4%) AVMs were located along the extremities and 3/21 (14.3%) AVMs on the trunk (Fig. 2). Cho’s classification [8] showed mostly type IIIa (11/19, 57.9%) and type IIIb (8/19, 42.1%). Regarding Schobinger classification [9], 2/21 (9.5%) were categorized as stage 2, 18/21 (85.7%) patients as stage 3, and 1/21 (4.8%) as stage 4. Eleven (52.4%) patients had undergone previous treatment, including incomplete embolization (11/21, 52.4%) and/or partial surgical resection (7/21, 33.3%).
Table 1 Comparison of BEST vs. BEET in AVMsFig. 1
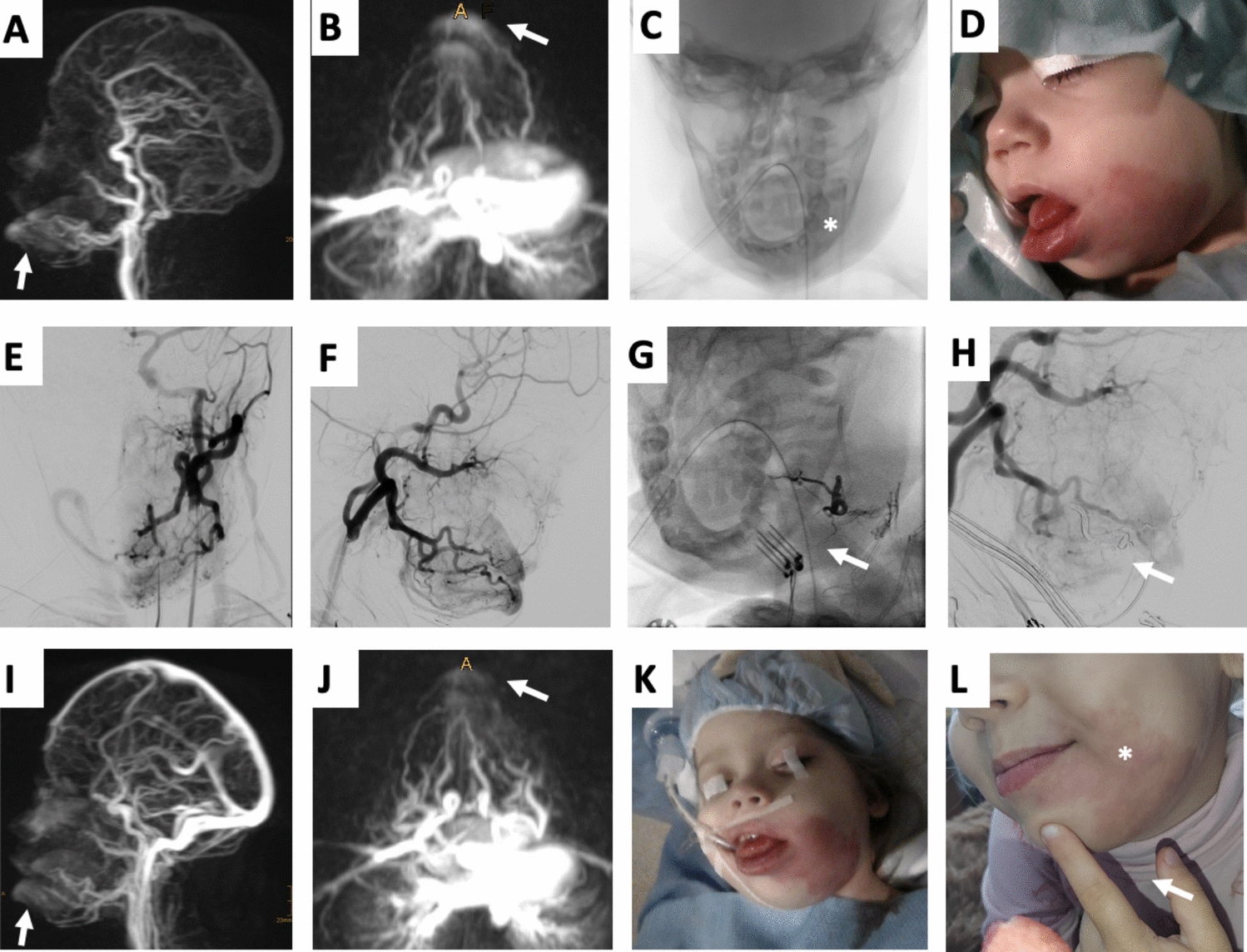
One-year-old female patient with capillary malformation-arteriovenous malformation (CM-AVM) syndrome presenting CMs on various localizations, an AVM on the left cheek as well as an osseous hyperplasia of the left mandibula undergoing two sessions of Bleomycin Electrosclerotherapy (BEST). A, B, MR-angiography presenting relevant fast-flow shunting of the vascular malformation on the left cheek involving tongue, gingiva, and lips (arrows). C, Digital subtraction angiography (DSA) image demonstrates an accompanying osseous hyperplasia of the left mandible (asterisk). D, Clinical presentation of the patient prior to treatment including noticeable swelling of the affected region and pink discoloration of the skin due to the arterial component in this lesion. E, F, DSA images before BEST revealing detailed vasculature architecture including angiographic classification (Cho type IIIa). G, H, DSA image during BEST procedure verifying electrode placement (arrow, I) as well as after BEST presenting immediately reduced AVM perfusion (H). I, J, MR-angiography showing reduced fast-flow shunting of the AVM (arrows) compared to A and B. K, Clinical presentation of the patient immediately after the second session of BEST at the age of two years. L, Clinical presentation of the patient at the age of three years, note the significantly reduced swelling and weakened pink discoloration
Fig. 2
Thirty-nine-year-old female patient with arterio-venous malformation (AVM) of shoulder undergoing two sessions of Bleomycin Electroembolotherapy (BEET). A, MR-angiography presenting location and extension of the vascular malformation on the left shoulder involving relevant fast-flow shunting (arrow). B, Clinical presentation of the patient prior to treatment including subtle pink discoloration of the skin. C, Digital subtraction angiography (DSA) demonstrates the vascular architecture of the lesion and microcatheter placement immediately before intra-arterial application of Bleomycin (arrow). D, DSA image during electroporation performed synchronously to embolotherapy. E, DSA image straight after BEET presenting significantly reduced lesion perfusion due to vascular lock phenomena. F, Clinical presentation immediately after BEET. G, MR-angiography three months after first BEET showing reduced fast-flow shunting of the AVM (arrow) compared to A. H, DSA image before admitting second BEET, notice the devascularization compared to C. I, J, DSA images during second BEET procedure verifying catheter (arrow) and electrode (asterisk) placement. K, Postprocedural DSA image demonstrates further reduced lesion perfusion. L, Clinical presentation of the patient one year after the second BEET, with slight postprocedural skin discoloration on the electroporation site (arrow) persisting at 6 months
Procedural CharacteristicsThirteen (61.9%) patients received one BEST/ BEET procedure, 6/21 (28.6%) patients received two, and 2/21 (9.5%) patients received three procedures (mean 1.5 ± 0.7 procedures). The mean number of electroporation cycles per treatment was 20.6 ± 13.1, in the BEST subgroup 23.1 ± 15.0, and in the BEET subgroup 18.0 ± 10.8. The mean dose of bleomycin was 8.9 ± 5.9 mg per session, in the BEST subgroup 10.6 ± 5.2 mg, and in the BEET subgroup 7.1 ± 6.2 mg (Supplemental Table 2).
Safety and ComplicationsPostprocedural complications were reported after 7/31 (22.6%) procedures (grade 2–3), including excessive swelling at the electroporation site (4/31, 12.9%, grade 2), postprocedural hematoma followed by delayed wound healing, solved by split-skin transplantation (1/31, 3.2%, grade 3), and persistent scarring in the treated area on the cheek not requiring surgery (1/31, 3.2%, grade 4). One patient with a facial AVM demonstrated jaw pain when chewing after BEET, completely regressing within 6 months without any additional measures (1/31, 3.2%, grade 2). Postprocedural skin discoloration limited to the electroporation site occurred after 14/31 (45.2%) procedures, in all cases fading in the postprocedural course though still visible at 6-months follow-up.
OutcomeThirteen (61.9%) patients showed partial relief of symptoms, 4/21 (19.0%) patients presented symptom-free, 2/21 (9.5%) without improvement of symptoms, and 2/21 (9.5%) with clinical progression (in both cases confirmed by MRI). MRI was available in 16/21 patients. In children ≤ 4 years (n = 4) of age, whose lesions were easy to monitor by ultrasound, no MRI was performed at follow-up. Substantial devascularization (76–99%) and partial devascularization (51–75%) were assessed in 6/16 patients (37.5%), respectively. Progression of the lesion was found in 3/16 patients (18.8%) and complete devascularization in 1/16 patients (6.3%).
Subgroup Comparison of BEST vs. BEETTen (47.6%) patients were treated by 16/31 (51.6%) BEST procedures, 11/21 (52.4%) patients by 15/31 (48.4%) BEET procedures (Table 1). The comparison of clinical outcome differed between both subgroups (p = 0.04); exemplarily, 4/11 (36.4%) patients treated by BEET rated symptom-free, while 0/10 (0.0%) patients treated by BEST did so. There were no significant differences in lesion devascularization on MRI (p = 0.28), though progression was only observed after BEST (3/9, 33.3%).
Comments (0)