
Remember me




First and foremost, the authors are to be commended for their timely and proactive approach in addressing the treatment of liver tumours larger than 3 cm, building upon the recent paradigm shift in the treatment of small-sized colorectal liver metastases (CRLM) (0–3 cm) established by the COLLISION trial [1, 2].
Tumour size remains a critical consideration in the field of thermal ablation. Historically, a 3-cm maximum tumour size was widely adopted as a standard, stemming from an era of less-advanced technology where local tumour progression (LTP) frequently occurred [3]. However, the field has since progressed considerably. Higher-power and wavelength-controlled antennas, phased or multi-antenna systems, and multi-electrode configurations, combined with feedback-controlled generators and waveform modulation, have enabled larger and more spherical ablation zones. Additionally, the use of hepatic artery catheters, stereotactic systems, and robotic guidance have improved visibility and targeting [4]. Perhaps most critically, the integration of confirmation software has fundamentally enhanced the ability to ensure complete tumour ablation [5]. As a result of these innovations, thermal ablation has gained widespread acceptance as a non-invasive, treatment with curative intent. Given its substantially lower complication rates compared to surgery and reduced LTP rates, these advances raise the question of whether thermal ablation should also be considered for patients with larger tumours [2,3,4].
The study’s findings are particularly insightful. The authors investigated patients treated with the HepACAGA technique between January 2021 and June 2025 [1, 4]. The cohort included patients with either CRLM or hepatocellular carcinoma (HCC), stratified into three size-based groups: 187 tumours ≤ 2 cm, 52 tumours of 2–3 cm, and 26 tumours of 3–5 cm. While the 1-year LTP-rate was most favourable for smaller tumours, no significant difference in LTP-free survival (LTPFS) was observed among the groups. Of the 13 LTPs reported, 12 were associated with inadequate margins despite using real-time margin confirmation. According to the authors, adequate margins could not be achieved in 4 of the 12 cases due to the proximity of critical structures, raising the question of why the margins were not achieved in the remaining 8.
Although LTP rates were highest in the group with larger tumours (8%; 2/24), they compare well to results from the COLLISION trial for both ablation (7%) and resection (8%) [2]. The finding that, despite longer ablation times and higher-power settings, LTP rates increase with tumour size, highlights a critical issue: ablation of larger tumours is inherently different from that of smaller tumours. This is emphasized by the fact that, although the overall number of complications was low, it was still highest in this subgroup [2, 3].
While the study is limited by the small sample size of the 3–5-cm tumour group, a relatively short median follow-up time and the inclusion of both HCCs and CRLMs, which may reduce statistical power and generalizability, questioning the 3 cm size threshold is highly relevant and paves the way towards expanding indications for curative-intent ablation of liver tumours, particularly those considered difficult to resect.
To conclude, the combination of (CB) CTHA guidance, higher-power systems, and real-time margin confirmation appears to be highly effective and safe when treating patients with CRLM and HCC across a broad range of tumour sizes. In an era of rapid technological progress in interventional radiology, especially in thermal ablation, further research is needed to push the boundaries of current treatments and provide patients with optimal, individualized, non-invasive options. The findings of this study, considered alongside ongoing trials such as COLLISION-XL, which aims to validate thermal ablation against SBRT for unresectable intermediate-size tumours (3–5 cm), provide strong evidence that the 3-cm tumour size cutoff should be reconsidered for unresectable tumours [1, 3, 6] (Fig. 1).
Fig. 1
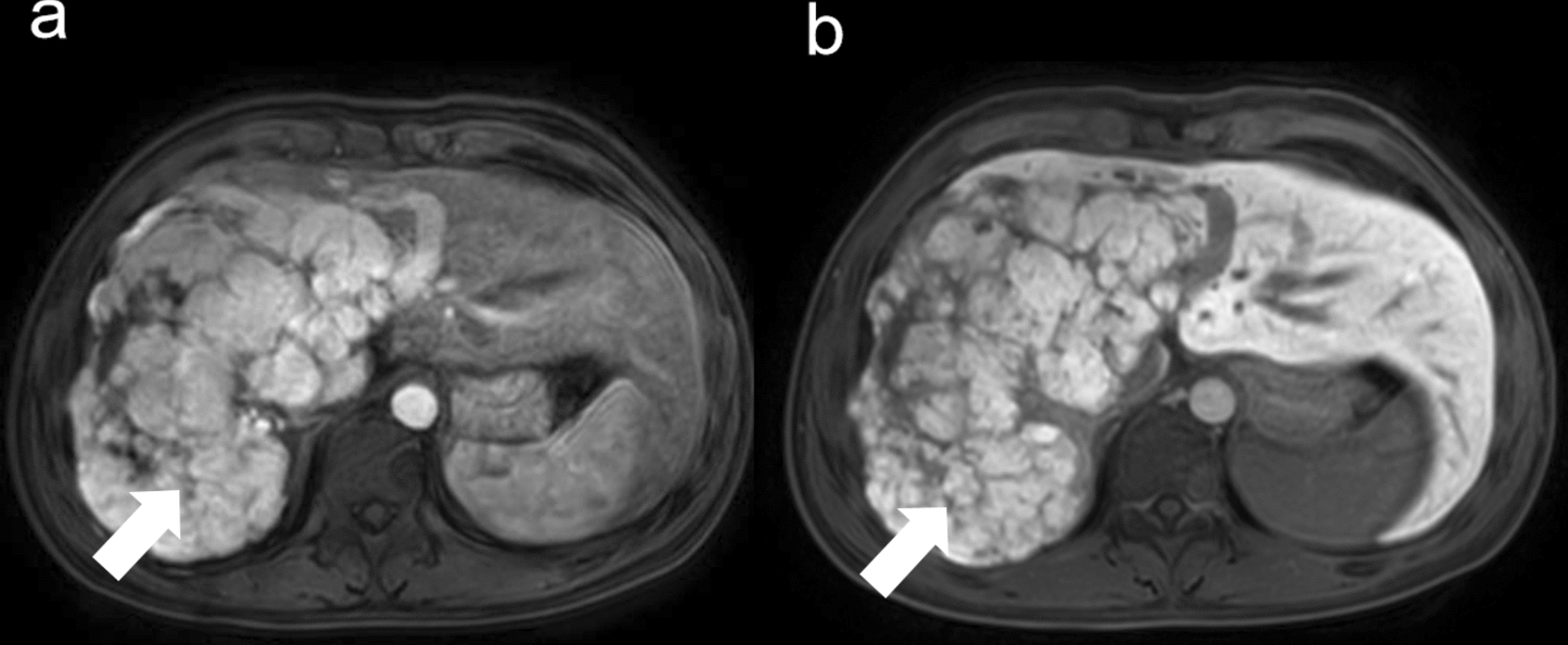
Example of a patient with a 5-cm colorectal liver metastasis (CRLM) treated with microwave ablation (MWA) in the setting of the COLLISION-XL randomized controlled trial. A and B. Baseline diffusion-weighted imaging (DWI)-MRI and contrast enhanced (ce)CT. C. Periprocedural CT showing the multi-antenna MWA. D and E. Follow-up DWI-MRI and ceMRI at 3 months. F. One-year follow-up 18F-FDG PET-CT showing no signs of local recurrence
Comments (0)