Despite the rising burden of HF in Japan, most predictive models are based on Western populations, limiting their relevance. Our study is the first to develop and validate a BNP-based HF risk score specifically for the Japanese population using prospective data from the Suita Study. Our results showed that older age, heavy smoking, former and heavy alcohol consumption, elevated blood pressure, eGFR < 45 mL/min/1.73 m2, history of CVD, cardiac murmur, arrhythmia, and LVH were associated with a higher risk of developing BNP levels ≥ 100 pg/mL among the Japanese general population. Given that BNP levels ≥ 100 pg/mL indicate HF that requires treatment [6], the above-mentioned risk factors may also predict future HF events. Based on these risk factors, we created a risk score to predict the possibility of developing BNP levels ≥ 100 pg/mL within the next eight years, which can be used to predict HF.
Our findings are consistent with those of Western studies that examined the risk factors for HF. In a pooled analysis including 24,675 participants from the original and offspring cohorts of the Framingham Heart Study (FHS), the Prevention of Renal and Vascular Endstage Disease (PREVEND) study, and the Multi-Ethnic Study of Atherosclerosis (MESA), male sex, obesity, hypertension, diabetes, smoking, AF, and previous myocardial infarction (MI) were associated with a higher risk of HF [12]. In a large cohort study of 871,687 individuals from the UK registered in the CArdiovascular research using LInked Bespoke studies and Electronic health Records (CALIBER) study, age, social deprivation, smoking, sedentary lifestyle, diabetes, AF, chronic obstructive pulmonary disease, BMI, hemoglobin, white blood cell count, and creatinine were associated with increased HF risk [14]. Using self-reported data from 5761 participants registered in the National Health and Nutrition Examination Survey (NHANES), older age, obesity, hypertension, diabetes, and CHD were identified as risk factors for HF [16].
In Japan, a retrospective cohort study involving 5335 rural residents from the Circulatory Risk in Communities Study (CIRCS) concluded that BMI of 27-29.9 and ≥ 30 kg/m2, systolic blood pressure ≥ 160 mmHg, diastolic blood pressure ≥ 100 mmHg, diabetes, and smoking ≥ 20 cigarettes/day were associated with a higher risk of pre-HF or symptomatic HF based on pro-BNP (NT-proBNP) [28]. The Fukuoka Diabetes Registry, a hospital-based study, showed that age, male sex, uncontrolled diabetes, serum adiponectin, sarcopenia, and CVD were risk factors for HF hospitalization in patients with diabetes [29].
In addition, a few Japanese studies investigated the associations with elevated BNP levels without assigning cut-offs for HF diagnosis. In a cross-sectional study involving 686 Japanese people, elevated plasma BNP levels were positively associated with age, female sex, higher blood pressure, urinary salt excretion, and high R-wave voltage, but inversely associated with hemoglobin levels [30]. Another cross-sectional study involving 8178 Japanese individuals from the Iwate-Kenpoku Cohort showed a positive association between elevated BNP levels and hypertension, major ECG abnormalities, history of CHD, and serum creatinine ≥ 1.2 mg/dL [31].
Notably, our study indicated that heavy smoking (≥ 40 cigarettes/day) was associated with an increased risk of developing BNP levels ≥ 100 pg/mL, while lighter smoking was not. Over half of the participants quit smoking during the follow-up period, potentially weakening this association. Data from 9345 participants registered in the Atherosclerosis Risk In Communities (ARIC) study showed that smoking cessation could significantly reduce HF risk [32].
Besides, we observed no association with obesity; a well-known risk factor for CVDs, including HF [33]. Previous epidemiological studies using data from the Suita Study and Western studies showed a negative correlation between BMI and BNP levels [34, 35], making it challenging to use BNP for HF diagnosis in overweight and obese patients [36]. However, BMI did not affect the association between other risk factors and BNP levels ≥ 100 pg/mL (p-interactions > 0.10), and BMI inclusion in the final regression model did not change the score.
Additionally, the lack of association with diabetes, another well-established risk factor for HF [37], might be attributed to the fact that most diabetic participants were receiving treatment, indicating that their condition was managed. Maintaining glycemic control may help prevent the onset and progression of myocardial dysfunction, thereby lowering the risk of HF events. Effective metabolic control has been associated with improved myocardial contractility, potentially due to more efficient use of energy substrates by the heart muscle and enhanced microvascular blood flow [38].
The developed risk score can be a practical tool for clinicians. By integrating age, smoking and alcohol use, blood pressure, renal function, CVD history, cardiac murmurs, arrhythmia, and LVH, the score may enable early detection of individuals at high risk of developing HF. It can also support preventive action through lifestyle changes or medical interventions. Building on our previous risk models for stroke, CHD, and AF [21, 39, 40], we aim to enhance the “Lifelong Health Support 10” program [41], which provides personalized health guidance. The newly developed risk score will be integrated into this program to further support targeted prevention efforts. We also plan to develop an online calculator based on this risk score to improve its clinical utility, allowing for quick and user-friendly risk estimation during routine healthcare visits.
Real-world scenario
Mr. Sato, a 76-year-old man, presents for a routine health check-up. He is a current heavy smoker (≥ 40 cigarettes/day), with a medical history of elevated blood pressure (155/95 mmHg), AF, cardiac murmur, and LVH on ECG. However, he experienced no major incidents of CVD, and his kidney function was normal (eGFR = 69 mL/min/1.73 m²). Using the BNP risk score system, he accumulates a total of 69 points out of 100 (Table 2). Referring to the chart, the incidence of elevated BNP rises steeply with higher scores, reaching over 50% for scores ≥ 60 (Fig. 2). Mr. Sato’s score places him in the highest risk category, indicating a one-in-two chance of developing BNP levels ≥ 100 pg/mL within the next years. This high score warrants a cardiology referral. In parallel, Mr. Sato should be advised on smoking cessation, blood pressure control, and adopting a heart-healthy lifestyle based on our “Lifelong Health Support 10” program [41].
Strengths and limitations
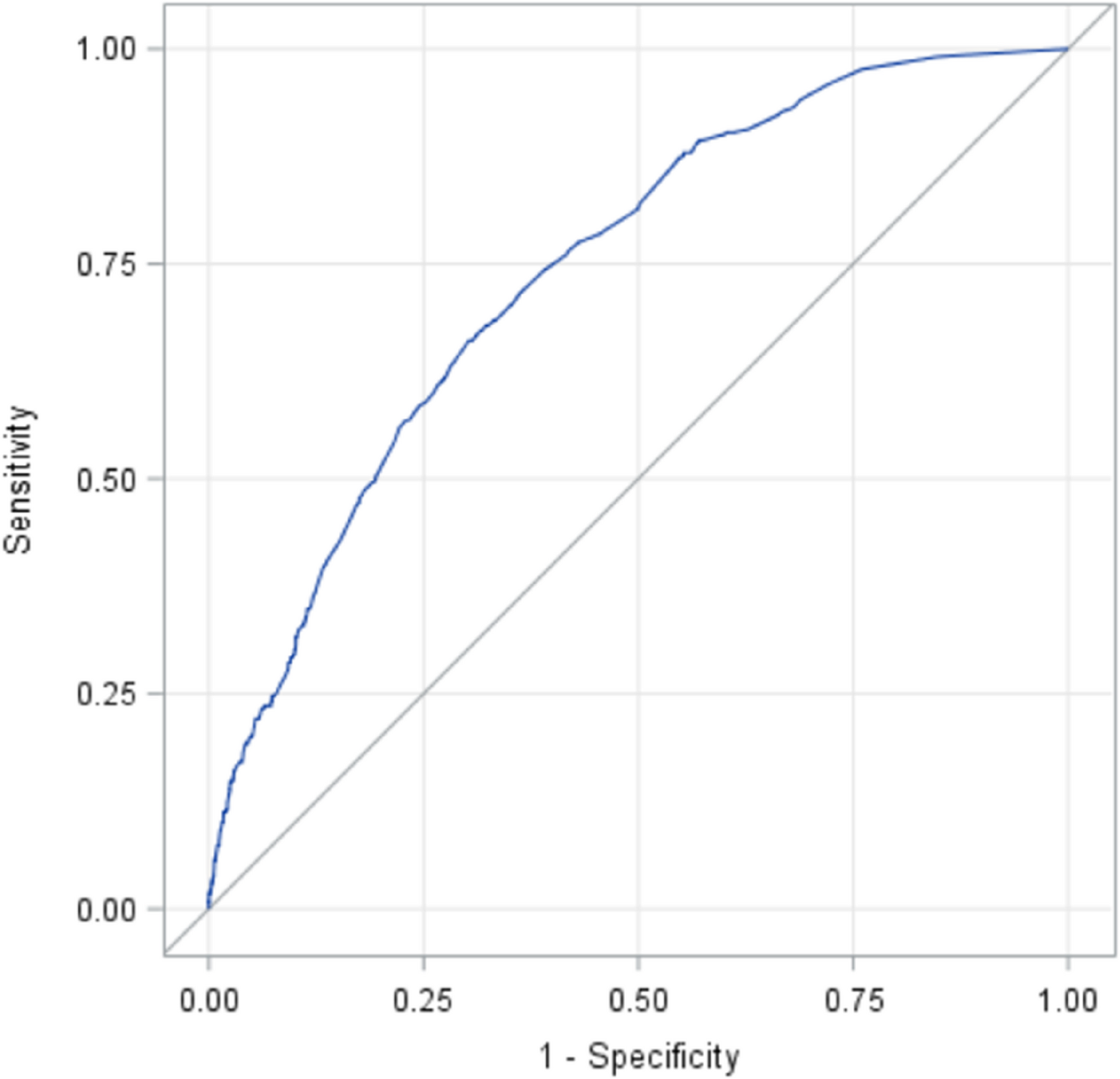
The main strengths of this study were investigating CVD risk factors for elevated BNP levels in a representative sample of the Japanese population, using a prospective design with frequent follow-ups, employing validated tools to assess risk factors, creating a prediction model with good discrimination and calibration, and developing a risk score.
However, this study had several limitations. First, although BNP levels are highly sensitive for diagnosing HF, many factors might reduce their diagnostic accuracy, such as age, BMI, AF, and renal diseases [7]. Therefore, a combination of clinical symptoms and echocardiographic findings is typically necessary for a definitive diagnosis of HF [3]. Second, the lack of echocardiographic data prevented the examination of the risk factors for different HF subtypes. Third, physical activity was assessed using a simple question that did not estimate the dose and intensity of activity. Fourth, LVH is typically diagnosed using a combination of clinical assessment, ECG, and cardiac imaging [42]. In this study, we solely relied on ECG. Fifth, we assessed the risk factors during baseline only. High-risk populations might have been closely monitored and treated, potentially leading to underestimating their risk. Besides, it could be suggested that measuring changes in clinical parameters, such as blood pressure, cholesterol levels, BNP concentrations, and eGFR, would minimize the risk of dilution bias. However, it is more practical in clinical settings and risk score calculations to apply risk factors collected at a single time point [43]. Sixth, the prediction model was not validated in different populations. Seventh, this study lacked data about medications that could interfere with HF management. For example, angiotensin receptor/neprilysin inhibitors (ARNIs) can reduce vasoconstriction, sodium retention, and maladaptive cardiac remodeling [44], and the PARADIGM-HF study demonstrated a superior efficacy of ARNIs over angiotensin-converting enzyme (ACE) inhibitors in reducing HF-related hospitalizations and mortality [45].

Comments (0)