Percutaneous coronary intervention (PCI) of calcified coronary lesions remains a clinical challenge, often resulting in suboptimal procedural outcomes and an increased incidence of MACE [1]. Effective treatment necessitates optimal lesion preparation prior to the implantation of the coronary stent, employing strategies such as pre-dilation with high-pressure non-compliant balloon catheters, modifying (cutting or scoring) balloons, or ablation techniques like RA and orbital atherectomy. Unlike RA, which primarily targets superficial calcified plaques, intravascular lithotripsy (IVL) effectively addresses both superficial and deeply calcified plaques [1].
The efficacy of RA or IVL has been the focus of several clinical studies. The findings of the most significant studies are displayed in Table 5. The Rotaxus study, which compared RA to standard lesion pre-dilation before paclitaxel-eluting stent (PES) implantation, revealed a higher early acute gain in the RA group but demonstrated significantly worse LLL at 9 months (p = 0.04). Importantly, differences in ISR, MACE, and TLR were not statistically significant. These results were consistent in the two-year follow-up, indicating no long-term clinical advantage of RA in this setting [6, 7].
Table 5 Summary of the most important studiesThe more recent Prepare-Calc study provided further insights into lesion preparation, comparing RA with cutting and scoring balloons (both followed by sirolimus-eluting stent). RA demonstrated a higher procedural success rate (p = 0.0001) and non-inferiority in 9-month LLL (p = 0.02), while the clinical outcomes, including TLR (p = 0.17) and target vessel failure (TVF; p = 0.78), were comparable between the groups [8].
In our study, a trend toward lower 12-month late lumen loss (LLL) was observed in the IVL group, with a p-value of 0.084. However, it is indeed a non-significant result and should therefore be interpreted with a caution. A plausible underlying mechanism may involve the ability of intravascular lithotripsy to disrupt not only superficial but also deeper layers of calcified plaque, thereby reducing the constrictive forces acting on the implanted stent. Conversely, the observation of negative LLL in some cases in the IVL group may reflect positive remodeling of the fractured calcified plaques, which could predispose to late stent malapposition.
On the other hand, we hypothesize that the higher (though not statistically significant) need for a second stent in the RA group may be due to more extensive (longer) dissections following rotational atherectomy.
The safety and efficacy of IVL have been evaluated in the Disrupt CAD I-IV studies, which highlighted its ability to achieve minimal residual DS% after stent implantation (7.8 ± 7.1%) and a high procedural success rate (92.2%) [2, 9]. In the Disrupt CAD III and IV studies, freedom from 30-day MACE was 92.4%, while 12-month MACE rates were 13.8% and 9.4%, respectively, with comparable reductions in target lesion failure (TLF) [10, 11].
We used angiographic inclusion criteria consistent with the Disrupt CAD studies. Only lesions classified as having severe calcification were included in our study. We also adopted the < 50% residual stenosis threshold based on the Disrupt CAD studies, which define procedural success in this manner. Using similar criteria enables comparability with previously published data.
Contrary, in our study, the IVL arm exhibited a slightly higher 12-month MACE rate (18.5%), primarily driven by the need for TLR (14.8%), but this difference appeared to be statistically insignificant when compared to the RA arm (p = 0.422). All TLRs in our study were ischemia-driven.Two in-hospital MACE were observed in the IVL group. The first involved a coronary artery rupture that did not occur during the lithotripsy itself, but rather during the subsequent post-dilatation with a non-compliant balloon, which was necessitated by a persistent significant waist. Emergency pericardiocentesis and surgical repair were required. The patient survived without long-term sequelae. It may be hypothesized that the use of a higher number of lithotripsy pulses could have mitigated this complication. The second event concerned the occlusion of a calcified side branch ostium, which could not be protected with a guidewire. This likely resulted from the rupture and displacement of a calcified plaque during the lithotripsy procedure. We believe that the slightly higher, though statistically insignificant, occurrence of MACE, despite a trend toward lower 12-month LLL, is primarily attributable to the two periprocedural complications mentioned above, both of which occurred in the IVL group.
Recently published the ROTA.shock trial had a similar setting as our study (i.e., the authors compared IVL with RA); however, this study with 70 patients randomized 1:1 assesssed the immediately postprocedural outcomes. They found IVL to be non-inferior to RA in achieving minimal stent area (MSA) and stent expansion (p = 0.79) [12]. These results support IVL as an effective alternative or adjunct to RA for calcified lesion treatment.
In the ROLLER COASTR-EPIC22 study, IVL was found to be non-inferior to RA in terms of stent expansion (Δ: −0.8; 95%CI: −6.5 to 4.8). In contrast, excimer laser coronary angioplasty (ELCA) did not demonstrate non-inferiority compared to RA (Δ: −6.1; 95%CI: −11.9 to −0.4) [13]. Both studies employed optical coherence tomography, which indeed represents a more advanced and accurate method for lesion assessment and stent optimization.
Rather than viewing RA and IVL as competing techniques, they may serve complementary roles, as exemplified by the “RotaTripsy” approach. This hybrid strategy employs smaller rotablation burrs (1.25–1.5 mm) to modify superficial calcifications and enable IVL balloon catheter delivery for addressing deeper calcium deposits. In our study, the “RotaTripsy” approach was used in two patients in the IVL arm due to uncrossable lesions. Additionally, IVL was employed in one patient in the RA arm due to stent underexpansion, a scenario increasingly documented in case reports and registries. For example, the SMILE registry demonstrated an 87.1% success rate for IVL in underexpanded stents, bringing significant improvements in MSA (p < 0.00001) [14].
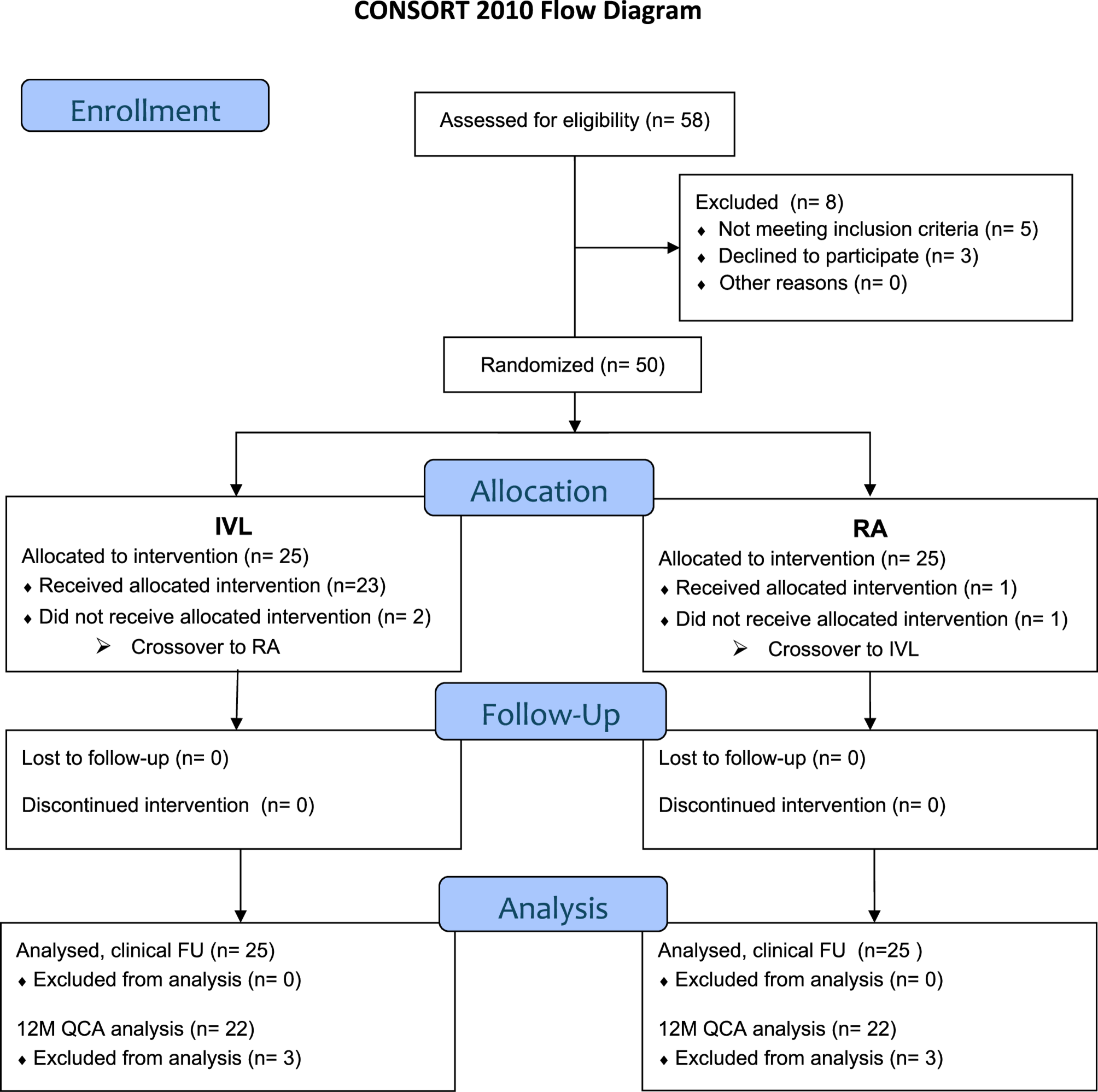
In all three crossover cases in our study, both early postprocedural and long-term clinical outcomes were favorable, with no incidence of MACE during follow-up. Although the necessity for crossover between treatment modalities was classified as procedural failure, the overall study analysis adhered to the intention-to-treat principle, thereby preserving the methodological integrity and minimizing bias in the comparison of treatment strategies.
Further comparisons of IVL and RA from retrospective studies reinforce the advantages of IVL, including larger MSA in the STIFF study (p = 0.01) [15], higher virtual FFR after IVL in Gallinoro et al. (p = 0.024) [16], and fewer periprocedural complications after IVL in Zhao et al. (p = 0.027) [17].
Despite the fact that intravascular imaging allows for a more precise evaluation of calcified coronary plaques, we utilized the 12-month angiographic late lumen loss (LLL) as the primary endpoint, similarly to the Rotaxus and Prepare-Calc studies. This methodological choice was predetermined by the pragmatic design of the trial and the availability of resources at the time. An angiography has inherent limitations, including its inability to provide detailed information on plaque composition and the precise extent of vessel wall calcification. Furthermore, it does not allow for the assessment of stent strut apposition, vessel remodeling, or other subtle morphological changes that may influence procedural outcomes. In contrast, intravascular imaging techniques offer more accurate and comprehensive characterization of coronary lesions, which is particularly advantageous in the evaluation of heavily calcified vessels. Although angiography is less accurate in the assessment of calcified lesions, it does allow comparison with the earlier studies mentioned above.
Further, multiple clinical studies have demonstrated a significant correlation, particularly between angiographic paramethers, such as LLL or percentage diameter stenosis (%DS), and the incidence of target lesion revascularization (TLR) [3, 4].
Although our study represents a pilot investigation, it provides sufficient data to inform sample size and power calculations for future trials. Based on the observed results for the primary endpoint of procedural success, a post hoc power analysis was performed to estimate the minimum sample size required for a future, adequately powered study. Assuming a significance level of 0.05 and a statistical power of 0.80, and using the observed procedural success rates of 84.0% in the IVL group and 96.0% in the RA group, the analysis indicated that a minimum of 95 patients per group would be required.
Limitations:
Our study has some limitations that should be mentioned. One of them is that this study represents a pilot investigation characterized by a limited sample size, which inherently restricts the generalizability of the findings. To validate and expand upon these preliminary results, additional research involving larger cohorts and adequate statistical power will be required to ensure robust and reliable conclusions. The statistical power was not calculated prior to the patient recruitment, either; however, as this study was designed as pilot study and as at the time of its beginning, no data on which we could have based the study power calculations were available, this limitation could not be avoided. We acknowledge a potential selection bias due to exclusion of patients with extreme anatomical complexity or limited feasibility of imaging or follow-up, which may affect the generalizability of our results. Furthermore, the use of intravascular imaging could enhance understanding of the extent of calcified coronary lesions.

Comments (0)