
Remember me
While most sudden cardiac deaths are due to structural heart disease or cardiac ischemia, intoxications are rather rare and often unrecognized. Against this background long-term side effects of smoking are well known, while acute toxic effects are not as well characterized.
Case presentationWe report a case of oral nicotine intoxication with subsequent resuscitation. We saw a 35-year-old patient with an unremarkable own and family history. After 4 pack years of smoking he had ceased smoking in spring 2023 and thereafter occasionally consumed e-cigarettes. On New Year´s Eve 2023 he attended a party with his wife. To relieve nicotine withdrawal symptoms, he trickled cumulative 60 mg of the pure nicotine liquid (20 mg nicotine/ml) in his mouth mucosa in the early morning of January 1st. 30 min later the patient suddenly complained of palpitations, became unconscious, and required resuscitation. Following bystander chest compressions the first emergency ECG showed ventricular fibrillation, which was successfully defibrillated. The patient was intubated and brought to our Cardiac Arrest Center.
On admission, the patient’s first 12-lead ECG showed an early repolarization pattern with an AV block I° (PR interval of 240ms). First-degree AV block regressed rapidly, while the early repolarization pattern increased within 24 h before gradually regressing as shown in (Fig. 1)without disappearing completely. A coronary angiography excluded coronary heart disease. The patient was extubated without neurological impairment, cardiac MRI, thoracic and cranial CT were performed, which also showed no significant findings.
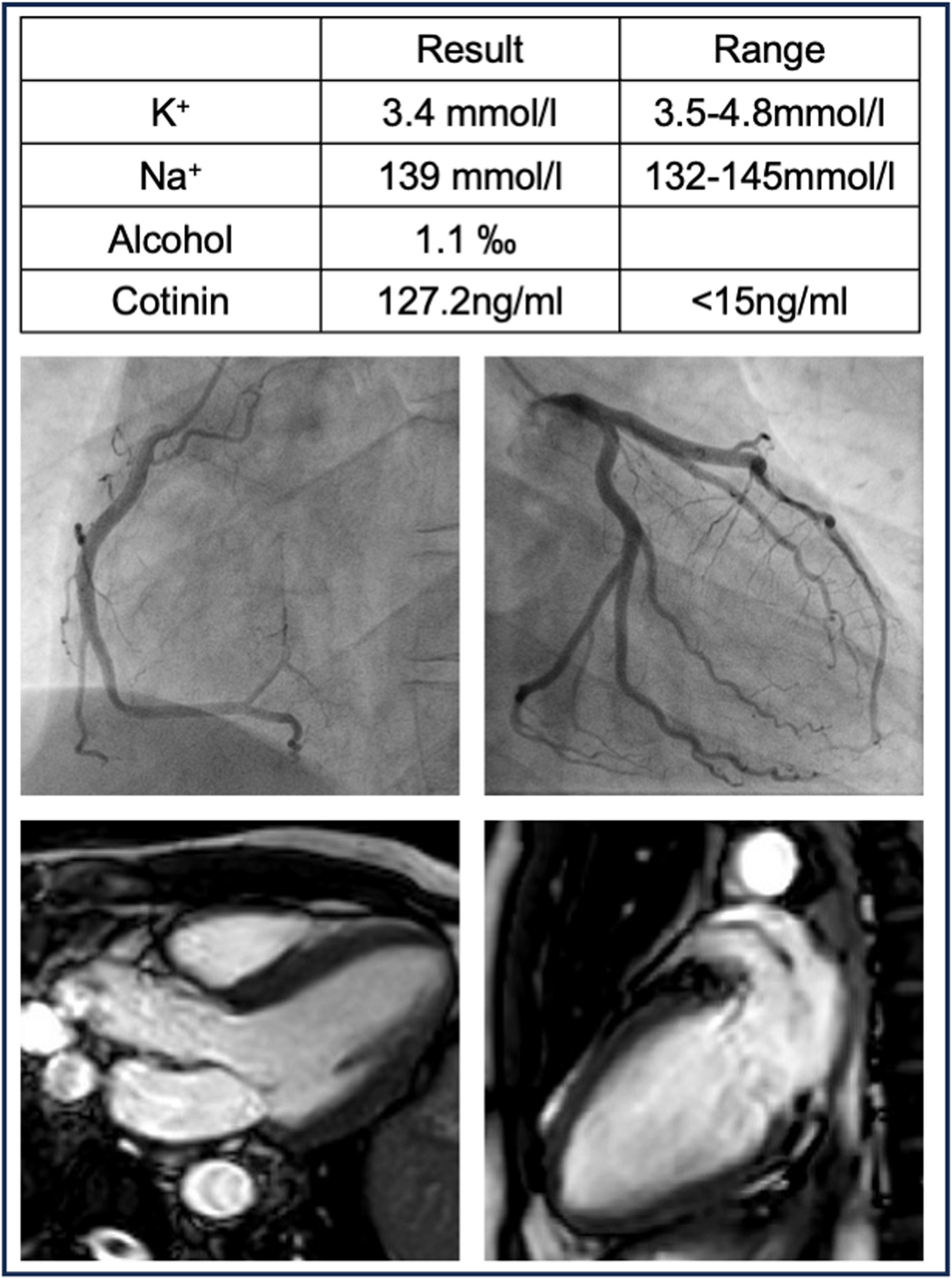
Fig. 1
Patient´s laboratory findings (upper row), coronary angiography (middle) and cardiac MRI (bottom)
Apart from a blood alcohol level of 1.1‰, the usual laboratory values were within the normal range. The level of the nicotine metabolite cotinine was 127.2 ng/ml (< 15ng/ml) in the gas chromatography-mass spectrometry, significantly above the usual limit. The remaining toxicological screening was negative (Fig. 2). In the course of the inpatient stay and under nicotine abstinence, the ECG changes regressed. Similarly, no arrhythmias were documented. Despite the nicotine-induced early repolarization syndrome with a most likely drug-induced resuscitation the patient and his wife decided on prophylactic therapy with a subcutaneous ICD. The patient was discharged after 8 days of inpatient monitoring. There were no new arrhythmias under nicotine-free conditions during follow up.
Fig. 2
Changes in the 12-lead-ECG following nicotine intoxication and sudden cardiac death (SCD). Asteriks indicate prolonged PR interval. Red arrows indicate prominent early repolarization pattern. Paper speed: 50mm/s, voltage: 10mm/mV
Comments (0)