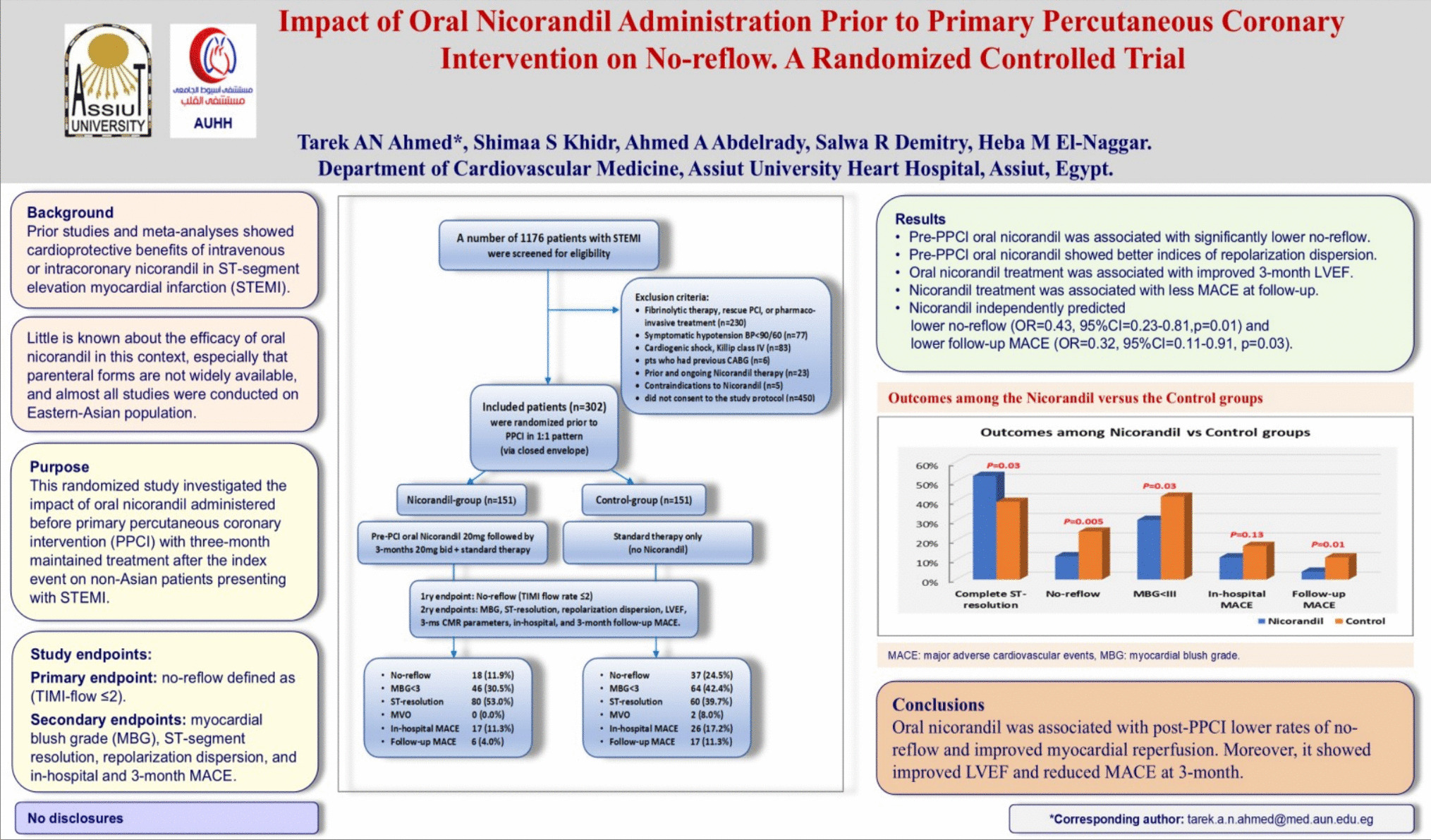
This study represents the largest randomized trial of pre-PPCI oral nicorandil in non-Asian STEMI patients. The main results of our study demonstrated that pre-PPCI treatment of STEMI patients with oral nicorandil was associated with significantly lower rates of no-reflow (11.9% vs 24.5%), better MBG, complete ST-resolution, and better repolarization dispersion with subsequently less ventricular arrhythmias compared to control. Oral nicorandil treatment was also associated with significantly improved LVEF and lower follow-up MACE.
Ideal management of STEMI involves timely reperfusion therapy via PPCI to restore normal coronary flow as a top priority, thus ensuring adequate myocardial tissue perfusion [1]. In this context, several adjunctive therapies have been tested. Previous trials failed to show significant benefit of upstream administration of GP IIb/IIIa inhibitors on microvascular reperfusion [1, 17]. Contemporary data on the upstream use of potent P2Y12 antagonists showed conflicting results [18, 19]. On the other hand, studies investigating upstream anticoagulation before PPCI [20], and other upstream medications including high-dose statin [21, 22] and Glucagon-like-peptide-1 (GLP-1) receptor agonist liraglutide [23] showed favorable impact on the microvascular function via their pleiotropic effects.
Nicorandil emerged as a promising therapeutic approach to preserve coronary microvascular integrity through its multifaceted nitrate-like and potassium channel opening properties [4, 5]. Previous studies demonstrated that pre-PPCI intravenous or intracoronary nicorandil improved microvascular dysfunction and reduced reperfusion injury [6,7,8,9, 24, 25]. However, little is known whether pre-PPCI oral nicorandil and maintained treatment thereafter would exert the same benefits, and whether it would influence clinical outcomes post-STEMI.
Our study hypothesized that early administration of oral nicorandil concomitantly with the standard pre-PPCI guideline–recommended antiplatelets in the emergency department, before transfer to the Cath lab for PPCI, would primarily lower the rates of reperfusion injury. This in turn would improve myocardial perfusion, limit the infarct size and rates of fatal arrhythmia, and ultimately improve clinical outcomes.
Impact of oral nicorandil on the primary outcome of no-reflow
Oral nicorandil is quickly and almost fully absorbed through the gastrointestinal system, reaching peak plasma levels within 30–60 min. It does not go through first-pass hepatic metabolism, unlike organic nitrates, with oral bioavailability more than 75%, and it is weakly bound to human plasma proteins (free fraction > 75%) [26]. Orally administered nicorandil at 15–40 mg led to a 36% reduction in coronary vascular resistance, increased coronary sinus blood flow up to 30%, and reduced LV end-diastolic pressure, thus improving coronary perfusion pressure [27]. Accordingly, it might provide a readily available alternative to the intravenous form which is not widely accessible.
Results of our study showed that the incidence of the primary outcome of no-reflow was 18.2%, which was significantly less among the Nicorandil-group compared to the Control-group (11.9% vs 24.5%, p = 0.005). Pooled meta-analyses of previous trials showed that intracoronary or intravenous nicorandil in the setting of STEMI significantly reduced the incidence of no-reflow with no heterogeneity [6, 7, 9, 13]. Our results showed significantly less frequent use of GP IIb/IIIa inhibitors among the Nicorandil-group, with no cases of deferred stenting, in contrast to 5 cases among the Control-group. This probably reflected the beneficial impact of pre-PPCI oral nicorandil administration on coronary flow in contrast to the Control-group which had higher rates of no-reflow and for which most operators tend to give GP IIb/IIIa inhibitors. Rates of no-reflow among our randomized groups were consistent with the pooled incidence from a prior meta-analysis of studies among PPCI patients who received nicorandil versus control (8.1% vs 20.8%, respectively) [13].
The relatively high rate of no-reflow reported by our study might be attributed to the higher proportion of anterior STEMI (66.9%) among our study population, entailing larger jeopardized myocardium, as well as relatively high rates of heavy thrombus burden (grades 4–5) (58.6%). Our results showed that both anterior STEMI and high thrombus burden were significant predictors of no-reflow. On the other hand, our results reported a median total ischemic time of 5 h, whereas the mean door to wire crossing time was only 43 min. This underscores that pre-hospital delay was the main contributor to the relatively long TIT observed in our study, which might be explained by the fact that our institute is a tertiary center receiving cases from remote rural districts whereby transportation would take some time. Despite this relatively long TIT, it was comparable among both randomized groups as well as among the no-reflow and normal flow groups and showed non-significant results regarding its possible predictability for no-reflow. Our results were concordant with the sub-analysis from the Total-trial that showed no difference in rates of no-reflow with symptom onset < or ≥ 6 h [2].
A prior study among ACS patients showed that single oral pre-PCI nicorandil (10–20 mg) was an independent protective factor against peri-procedural myocardial injury [11]. On contrary, a previous trial on pre-PPCI oral nicorandil failed to show beneficial effects on either coronary blood flow or ST-resolution [28], which might be attributed to their use of a double dose (40 mg) that could negatively impact the patient’s hemodynamic status due to the exaggerated hypotensive effect.
Moreover, our results showed that pre-PPCI oral nicorandil was associated with significantly higher rates of complete ST-resolution (53.0% vs 39.7%, p = 0.03) and better MBG (69.5% vs 57.6%, p = 0.03), reflecting better tissue microcirculation perfusion compared to the Control-group. This was concordant with the results of a previous study using intracoronary nicorandil [29], and results of a pooled analysis of 10 studies whereby nicorandil was associated with complete ST-resolution with no heterogeneity [9].
Despite that TIMI flow grade, myocardial blush grade, and ST-segment resolution are used as surrogate measures of myocardial reperfusion following PCI, yet they reflect different perspectives of the reperfusion process. This might explain the discrepancy noted in our study between complete reperfusion as suggested by coronary blood flow (TIMI-III was 81.8%), visually assessed myocardial perfusion grade (MBG-III was 63.6%), and complete ST-segment resolution (46.4%, defined as STR ≥ 70% at 90 min post-PPCI). It was previously demonstrated that improved coronary blood flow (TIMI-III) does not necessarily imply restored tissue level perfusion [14]. A prior study of 5966 patients with STEMI showed ≈20% discrepancy between TIMI flow grade and ST-segment resolution (successful ST-resolution was defined as resolution of ≥ 50% assessed 120 min post-PPCI), whereas an integrated analysis of both showed incremental prognostic benefit [30]. An earlier study showed a slight association (kappa = 0.55) between MBG (which reflects microvascular integrity) and STR (which reflects myocyte integrity) [31]. Thus, a comprehensive assessment that integrates all three measures (TIMI flow, myocardial blush, and ST-segment resolution) better reflects myocardial salvage and successful reperfusion following PPCI, emphasizing complementary rather than supplementary role of these measures. Our results collectively elucidated the benefit of pre-PPCI oral nicorandil on enhancing myocardial recovery post-PPCI both at epicardial and microvascular levels.
Impact of oral nicorandil on repolarization dispersion and arrhythmias
While ST-segment resolution is an established measure for myocardial reperfusion, repolarization dispersion indices are less established. Nevertheless, assessment of repolarization dispersion has gained interest as a reflection of impaired myocardial reperfusion and subsequent inhomogeneity in ventricular repolarization which might predispose to serious arrhythmic events.
Nicorandil, as a K+-channel opener, reduces calcium overload in the vulnerable ischemic myocardium, resulting in suppression of ventricular arrhythmias [4]. In an early small-scale study, it was demonstrated that pre-PCI treatment with oral nicorandil among patients with stable angina reduced QTd [32]. Later this cardioprotective role of nicorandil, in terms of ventricular arrhythmias, was demonstrated among STEMI patients undergoing PPCI [8, 33].
Our study showed marginally significant better indices of repolarization dispersion and numerically less ventricular arrhythmias among the Nicorandil-group. A previous randomized study of 120 STEMI patients showed that those receiving pre-PCI oral nicorandil 10 mg followed by 15 mg/day for 3 days had significantly lower QTd and less ventricular premature beats and VT/VF than the Control-group [34]. Noticeably, they assessed QTd at several time points throughout the 3 days of admission starting at 6 h, unlike our study which assessed repolarization dispersion at a single time point (90 min post-PPCI). Moreover, they used continuous ECG monitoring for the assessment of ventricular arrhythmias, which permitted the detection of non-sustained arrhythmias.
Impact of oral nicorandil on infarct size and myocardial function
The beneficial effects of nicorandil extend to involve infarct size and myocardial function. An experimental animal study showed that the administration of nicorandil prior to coronary microembolization reduced myocardial cell apoptosis, with subsequent enhancement of cardiac function [35], and post-ischemic myocardial regeneration with a considerable dose-proportionate decline in infarction size [36]. Pre-PCI intravenous nicorandil among STEMI patients was shown to be associated with non-significant difference in LVEF after 1 week but demonstrated significantly greater LVEF at 6 months compared to control [37].
Moreover, a large-scale multicenter trial conducted in Japan showed that although IV nicorandil did not affect infarct size estimated by CK levels, or LVEF at follow-up, the subset of patients who were given nicorandil orally in the chronic phase had a greater increase in their LVEF [38]. Similarly, our results showed that although pre-PPCI nicorandil did not influence the infarct size estimated by CK or troponin levels as well as in-hospital LVEF, continued nicorandil treatment demonstrated significantly better LVEF and WMSI at follow-up. It is worth noting that in our study with the lack of serial assessment of the cardiac enzymes, we might have missed peak troponin levels which better reflect infarct size.
On the other hand, our results demonstrated significantly better MBG among the Nicorandil-group that might reflect smaller infarct size, despite the limitation of being visually assessed. It was previously demonstrated that quantitative blush evaluation (QuBE) correlates with infarct size and microvascular dysfunction by CMR [39] and that low QuBE score significantly predicts larger infarct size and reduced LVEF among patients with STEMI who underwent PPCI [40].
A prior larger randomized study showed that early use of IV nicorandil prior to PPCI resulted in an increased LVEF and reduced myocardial infarct size on CMR [16]. However, unlike ours, their study was powered to the primary CMR outcomes. In our study, although the Nicorandil-group showed numerically better CMR data in terms of lower percentage of enhanced LV volume, microvascular obstruction, and better LV volumes and EF, the difference was statistically non-significant. This might be attributed to the small, underpowered CMR sample size.
Impact of oral nicorandil on MACE
Regarding the impact of oral nicorandil on MACE, our results showed that it was associated with and independently predicted 3-month MACE-free survival, mainly derived by reduced HF hospitalization. Likewise, Feng et al. [8] showed reduced incidence of HF rehospitalization and overall MACE among patients receiving nicorandil at 6-month follow-up. This was consistent with the results of a prior meta-analysis which showed that drugs targeting mitochondrial function when used as an adjunct to PPCI, reduced HF hospitalization [41]. Results from the Korea Acute Myocardial Infarction Registry (KAMIR) showed that patients who received IV or oral nicorandil on admission followed by maintained oral nicorandil for 6 months had a significant decrease in 1- and 6-month composite MACE, death, and recurrent MI [42]. This highlights the notion that the benefits of nicorandil extend beyond the acute phase of MI.
Data from a previous study showed lower all-cause mortality rates among patients who received oral nicorandil at discharge following acute myocardial infarction [12]. On the contrary, our study showed no mortality benefit for oral nicorandil either in-hospital or at 3 months. Our results were in accordance with the results of a previous meta-analysis of 14 RCTs comparing nicorandil treatment prior to PPCI with control, which showed that despite the findings that nicorandil treatment reduced no-reflow, increased LVEF, and reduced the incidence of ventricular arrhythmia as well as congestive heart failure, yet no difference in mortality was observed [7]. Similarly, a more recent meta-analysis of 18 RCTs showed that nicorandil administration was significantly associated with less MACE, mainly derived from less HF hospitalization and ventricular arrhythmia, but not mortality. This benefit in terms of MACE was more obvious among patients maintaining nicorandil after PPCI [9].
Given the limited worldwide availability of intravenous nicorandil, more information about oral nicorandil in the pre-PPCI phase among acute STEMI patients might be warranted. Randomized trials assessing the use of oral versus intravenous/intracoronary nicorandil in this setting and powered to longer-term clinical and LV functional endpoints might be needed.
Limitations
This was a single-center, open-label study. Baseline CMR was not performed due to financial and logistic constraints, yet a 3-month CMR was performed with the assumption that it would reflect the impact of maintained nicorandil therapy. However, CMR results were inconclusive probably due to the small subset of patients (n = 50) who underwent assessment. Additionally, our study was not powered to detect secondary outcomes of microvascular obstruction or clinical events and was limited by short-term follow-up. Finally, we did not report on the incidence of side effects of oral nicorandil; however, the low rates of patients who have dropped out of nicorandil treatment indicate that it was well tolerated.



Comments (0)